L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Inserts-rev1(10/30/01)
Second-hand Aerosols in Acute Care Therapist Exposure Risk and the Potential Impact of Device Selection. *A Brief Review of the Literature on Second-hand Aerosols and the Effects of Occupational Exposure • Danger in the Air, Proctor S., Advance for Respiratory Care • Second-hand (S)-Albuterol: RT Exposure Risk Following Racemic Practitioners, January 24, 2005. Albuterol, Carnathan, et al. Respiratory Care, October 2001, V46,
In a review and expansion of the 2004 Chest article this publication
states "respiratory therapists are at an increased risk of developing
Whether exposure to nebulized medications such as Racemic
asthma and asthma-related symptoms due to their involvement in
Albuterol (RAC) contribute to increased incidence of asthma among
the diagnosis and treatment of patients with respiratory conditions."
respiratory therapists is unknown. This in vivo study was designed
In separate communications with the lead author, Advance reports
to determine if the S and R isomers in RAC are detectable in the
"Routine monitoring and care of patients can expose therapists to
plasma of RTs. After a two-day work holiday blood was drawn at
trace amounts of airborne agents that can trigger respiratory
baseline, 2, 4, and 8 hours after exposure on days 1 and 4. Subjects
symptoms and cause exacerbations of acute asthma;" and "Under
were exposed to an average of 31mg of RAC for 4.3 hours each day.
current conditions, control of exhaust aerosols is paramount. …
Results indicate RAC isomers increased with exposure. The study
this includes use of scavengers, developing shut-off devices for
concludes S isomer (proinflammatory effects) achieves higher
plasma levels (1.6 to 2.5 fold) than R isomer (confers all off the
bronchodilatory effects) and stays in the systemic circulation for a
• Respiratory Health Survey of Respiratory Therapists, Dimich-Ward,
Study showed that RTs have an elevated prevalence of asthma
• Asthma Risk and Occupation as a Respiratory Therapist,
diagnosis after they enter into the profession, and when compared
Christiana DC, Kern DG. American Review Respiratory Disease 1993,
to a control group of Physical Therapists, are more than twice as
likely to develop respiratory symptoms. The study also found that
A study of 2,086 respiratory therapists and 2,030 physical
the administration of specific aerosolized medications was
therapists found a history of physician diagnosed asthma in 16% of
associated with an increased risk of asthma.
respiratory therapists and 8% of control subjects. When analysis
was restricted to those who developed asthma after entry into the
profession, RTs still had a significant excess, 7.4% versus 2.8%. • Respiratory Therapists Twice as Likely to Have Asthma Than Other Therapists - Exposure to Patient Treatments May Increase
This article concludes efforts should be directed to identifying
Therapists' Asthma Risk, Canadian Society of Respiratory Therapists
potential agents responsible for this form of occupational asthma.
R.S. Irwin MD, FCCP, President of the American College of Chest
Physicians, quoted in the article states, "It is important for
respiratory therapists and other medical professionals to recognize
and understand the possible respiratory effects related to the
administration of aerosolized substances and take appropriate steps
to minimize their exposure to these medications during patient
• Mist-ical Problem - Aerosolized Patient Exhaust May Jeopardize Practitioner Airways, Advance for Respiratory Care Practitioners,
". evidence suggests some RTs are at risk of developing
occupational asthma when treating asthmatics. At issue is an
unintended consequence of liquid nebulization." Patrick Dunn,
quoted in the article speculates, "The higher than average
occupational asthma rate is probably related to passive inhalation of
the exhaust of patients' aerosolized medications. The reality is we
need to change the way nebulizers are designed. You are giving the
room a treatment." Manufacturers have responded to this emerging
need with filter attachments and nebulizers designed for low
environmental loss such as the AeroEclipse® breath-actuated
nebulizer that produces aerosol in response to the patient's
AeroEclipse ® II BAN - Breath actuation proven
These studies used the AeroEclipse® Breath Actuated Nebulizer, not the AeroEclipse® II Breath to reduce exposure to second-hand aerosol
Actuated Nebulizer (BAN) which is currently on the market. The AeroEclipse® BAN and AeroEclipse®
II BAN are equivalent in regards to in vitro performance.1
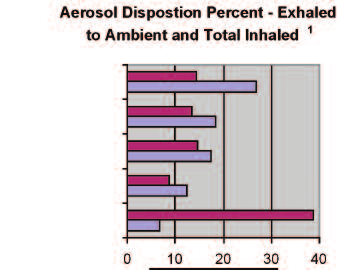
Changing the way nebulizers are designed can reduce the risk of second-hand aerosols. The AeroEclipse® II Breath Actuated Nebulizer (BAN) is engineered to reduce the environmental loss of aerosol. The literature supports the unique benefit of this SVN to reduce occupational exposure to second-hand aerosols. Performance Comparison of Nebulizer Designs: Constant-Output, Breath-Enhanced, and Dosimetric. Aerosol Disposition Percent - Exhaled
Rau, et al. Respiratory Care, February 2004, Vol 49 No 2,
to Ambient and Total Inhaled1
This study (also mass balance) evaluated the in vitro dose
disposition (delivered to patient, lost to the equipment and
lost to ambient) with 5 different nebulizer models representing
3 product types-constant output, breath-enhanced and
dosimetric-using simulated normal, adult breathing. Theresults concluded, "The nebulizers we tested differ signifi-
AeroEclipse® provided the largest inhaled drug mass and the
lowest loss to the ambient air …" (See chart at right.)
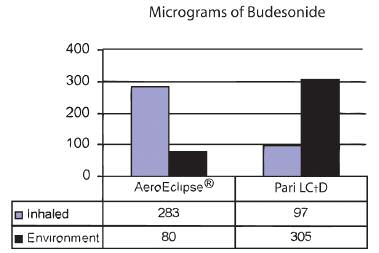
1 Study used 2.5mg Albuterol in 3ml fill volume. Delivery of a Suspension Corticosteriod Formulation by Small Volume Nebulizers: A Comparative Bench Study. Micrograms of Budesonide
Mitchell, et al. ERS Congress, September 2001, Abstract#290. • This study reports the in vitro delivery of 0.25% mg/ml
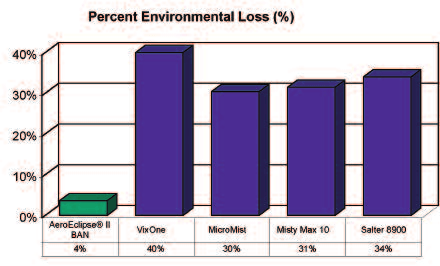
Budesonide suspension in two types of SVNs including the AeroEclipse® and Pari LC®D under simulated adult breathing conditions. The study reported total drug mass delivered to the patient and the environment. (See chart at right.) The authors conclude "The breath-actuation feature of the AeroEclipse® SVN minimizes aerosol release to the environment during exhalation, which may cause adverse effects to both patient and health care provider." Breath Actuated AeroEclipse® II Nebulizer: Performance Validation and Comparison to Competitive Products. Percent of Environmental Loss (%) • This study measures the in vitro environmental loss of the AeroEclipse® II BAN and competitive other small volume nebulizers including: Hudson MicroMist®, VixOne™, Airlife™ Charat to come
Brand Misty Max 10™ and the Salter 8900 Series. The study reported total environmental loss for each nebulizer based on 2.5mg Albuterol dosing. (See chart at right.) The findings conclude the AeroEclipse® II BAN delivers far less aerosol to the environement. As the AeroEclipse® II BAN delivers aerosol only on patient inspiration, the vast majority of the aerosolized drug goes to the patient and not into the environment.
1 ARE FIRST AND SECOND GENERATION, MECHANICALLY-OPERATED BREATH-ACTUATED NEBULIZERS (BAN) COMPARABLE BASED
J. Schmidt, J. Pevler, C. Doyle, K. Wiersema, M. Nagel. J. Mitchell; Respiratory Drug Delivery, 2006: 817-819.
™ and ® are trademarks and registered trademarks of Monaghan Medical Corporation or an affiliate of Monaghan Medical Corporation
† trademarks and registered trademarks of the respective companies
www.didactique.info/ioste - Tunisian Team Host Committee - ioste2007meeting@didactique.info VENUE, ACCOMMODATIONS & NOTE OF INFORMATION The Ioste meeting will be held in Yasmin Hammamet (South Hammamet), Tunisia, from Wednesday 07 to Saturday 10 February 2007 , and our Tunisian Team Host Committee is enthusiastically preparing for it. To contact us in Tunisia during the M
Institut für Medizinische Diagnostik Berlin – Potsdam MVZ GbRLaboratoriumsmedizin • Mikrobiologie • Infektionsepidemiologie • Humangenetik • Transfusionsmedizin Diagnostik-Info 288 Simvastatin-Intoleranz Optimierung der Statintherapie mittels SLCO1B1-Genotypisierung Statine wirken lipidsenkend, indem sie die Choleste- In Abhängigkeit vom SLCO1B1-Genotyp nimmt das r



 Second-hand Aerosols in Acute Care
Second-hand Aerosols in Acute Care



 Changing the way nebulizers are designed can reduce the risk of second-hand aerosols.
Changing the way nebulizers are designed can reduce the risk of second-hand aerosols.