L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Updatejan2006-org
Vol. 14 - No. 1 FOR PRIVATE CIRCULATION ONLY JANUARY 2006
Leprosy is regarded as a serious public health problem
special attention remained a niggling problem. The number
mainly because of the disabilities it produces in some of
of patients with disability presenting themselves at the
those affected with it. It is, therefore, regrettable that very
clinics was so many that leprosy continued to be regarded
little attention has been given to one of the principle facets
as a disease that produced horrifying disability and suffering.
of leprosy control, prevention of disability. Every year
This negative image contributed to stigma and discrimination.
about 1000 to 5000 new cases with disability are detectedin India. The numbers can at best be conservative since
Leprosy disease burden has come down thanks to the
there may be considerable underreporting of disability in
efforts of thousands of health workers. Transition from
some areas. The country is estimated to have one million
focused action by the vertical programme to intensified
patients with leprosy-related disabilities. Even if it is an
extension of MDT service coverage through the involvement
overestimation, as suggested by some, the number would
of the General health service has been smooth and has
not by any means be small. It is unfortunate that the
contributed to a large extent to the present leprosy situation.
leprosy-disabled are neglected by themselves, ignored by
While integration has brought in rich dividends it has also
their families and forgotten by the programme.
brought into focus unsolved problems in leprosy control.
of bandage, cotton and antiseptic cream was the
health staff with too many responsibilities which otherwise
'POD activity' carried out by the leprosy control staff at the
will impede them from participating in basic activities.
so-called mobile MDT clinics. Temporary hospitalisation
Prioritisation based on established levels of competence
wards established to address specially the disability problem
and on compulsion of reaching the predetermined target
succeeded in providing only temporary respite to a few
is understandable but this in no way should deter us from
patients. Management of persons with complications
looking at benefits from the individual patient's point of
including disabilities related to the disease was, therefore,
view. A programme which is more than 50 years old should
confined largely to specialised institutions mostly run by
be able to provide a broad spectrum of service that caters
Non Governmental Organisations (NGO). Since the number
to patients with different set of problems. There should be
of such institutions was limited, coverage of patients requiring
no room for excuses like, "They are not well-equipped to
Editorial Office : Damien Foundation India Trust, New No. 14, Venugopal Avenue, Spur Tank Road, Chetpet, Chennai 600 031.
Telephone: 2836 0496, 2836 1910 • Fax : 2836 2367 • E.Mail : damienin@vsnl.com, damienin@touchtelindia.net
Dr. P. KRISHNAMURTHY
deal with consequence of leprosy", "It is not
!It is unfortunate that a priority", "It is difficult to implement."
Prevention of disability should start with early
Associate Editor :
diagnosis and prompt treatment of incident
cases. It has been three years since integrated
Mr. D.V. PREMKUMAR VELU
leprosy service delivery was initiated. After
Advisers :
several campaigns and training sessions, both
Dr. CLAIRE VELLUT
formal and informal, general health staff appear
to be competent enough to manage leprosy. Dr. P. VIJAYA KUMARAN
But management of complications including
Dr. JACOB MATHEW
satisfactory. This is because of two reasons: the staff may not be competent to
Dr. T. PRABHAKAR RAO
manage complications and a back up referral system with centres to manage patientswith different problems is not yet established. There are reports of patients with
complications getting no treatment or getting treatment which is far from what is
minimally acceptable and expected. Chronic or recurrent reactions which are due
mainly to mismanagement of cases are becoming increasingly common. Since
about 15% of MB cases and 2% of PB cases are likely to get reaction there should
be a mechanism in place whereby these patients are identified timely and treated
promptly to avoid the development of deformities. Every Medical Officer in the
general health should be able to identify reaction but the treatment of reaction cases,depending on competence, may be the prerogative of the Medical Officer or referral
CONTENTS
foci within the district identified for this purpose. The referral centre may be the
district hospital or sub-district hospital or NGO project.
What do we do for patients already with deformities? The principal aim is to ensure
that the deformity does not deteriorate or it is as much limited as possible. Also the
possibility of reversing the deformity through reconstructive surgery should beexplored. For the first group of patients what is required is self care under the
guidance of health worker. Properly trained health worker will be able to providethe necessary guidance and counseling to patients with deformity so that they are
able to take care of their disabilities. Since in a district each health worker may hardly
have one to 5 cases with deformity it is not difficult for the worker to take up this
task. The patient can be monitored and provided guidance during the routine villagevisits at least once a month. District hospital could be trained to manage complicated
ulcers including septic surgery. Experience suggests that these things can be done
better with the involvement of an NGO as a facilitator. Trichy and Salem districts
in Tamil Nadu are standing examples of excellent collaboration between Governmentand NGO project which has resulted in the basic health workers in 20 PHCs in Trichy
and 30 in Salem taking up POD activity seriously and implementing prevention of
disability in their areas on their own (This will be extended to the remaining PHCsalso so that by the end of 2006 all the PHCs in these two districts will be fullyimplementing POD).
Each district in the country may have an average of 500 persons with leprosy-relateddisability (it may vary from 100 to 3000). At least 20% of them will be eligible forcorrection of their deformity. Since majority of tertiary care centres are confinedto the South, coverage is a serious problem. It is unfortunate that no major hospitalat the state headquarters has taken up this responsibility. There are very fewGovernment Institutions which are catering to the important segment of the community. Under the circumstance the establishment of reconstructive surgery service for
leprosy-affected persons at Medical College hospital inPatna and Dharbhanga in Bihar through the coordinated
effort of Government and Damien Foundation India Trust(DFIT) is indeed a laudable initiative. Surgeons and
physiotherapists in these two centres were identified by theGovernment and trained by the visiting surgeon and
physiotherapist from Damien Foundation India Trust. A
set of surgical instruments was provided. Cases requiringsurgery were continuously fed by the District TechnicalSupport Team through the District Leprosy Officer. Following
Finally, all the health facilities in the State should be provided
3 to 4 supervisory training visits by the visiting surgeon and
with the list of referral centres managing reactions or
physiotherapist the staff in the two centres are able to
disabilities or reconstructive surgery so that patients needing
manage patients on their own. Effort should be made to
specialised care could be referred to these centres for
establish at least one such centre in every State preferably
in a Government institution for the sake of sustainability. This is possible only if NGOs play the most important role
The aim of leprosy control should be the reduction not only
of facilitators rather than implementers. A network of tertiary
of disease burden but of disability burden too. This will
care centres run by Government or NGO across the country
have a positive consequence on the perception of the
would fulfill the needs of hundreds of leprosy patients with
disease by the community and improve the possibility of
their active participation in the programme.
Village Health Nurses bring meaning to leprosy affected
Holy Family Hansenorium (HFH) project which is located
The project adapted the two adjacent districts-Trichy
in Fathimanagar, a village about 18 Kms from Trichy town
and Pudukottai. The project first had a discussion
in Tamil Nadu, has been providing service to
with the District Leprosy Officer (DLO) and sought
leprosy-affected for the past five decades. The activities of
permission to facilitate POD in the district. The intentions
the project related to Leprosy and TB control are supported
of the project were not clear to the Government staff-
by Damien Foundation India Trust (DFIT). From Survey
they thought that the project was interested in taking
Education Treatment (SET) activities implemented in a
over leprosy control activities in the district. The field staff
field area allotted by the Government with hospital back-
from HFH had to overcome initially the suspicion
up support through a large workforce of unipurpose workers
in the minds of the vertical staff who were still possessive
to a programme, with limited staff, of supporting and
about the programme and reluctance on the part
strengthening the Government programme following
of the General health staff to take up 'additional
integration the journey for the project has been exciting
responsibility'. Persistence paid off. The project was asked
and gratifying. It has helped the Government in Trichy
to train the staff for implementing POD as per Government
district to establish Prevention of disability (POD) care
of India (GOI) guideline. The Medical officers and former
services. How the project has succeeded in accomplishing
this is an interesting story worth sharing.
In spite of that POD was not implemented in the districts.
(pot, stone, washed cotton ribbon cloth -for bandage-, oil)
Then the project with permission from the District Health
was the key intervention. The whole process took almost
Officer identified one block in each district to facilitate the
introduction of POD. The key field staff of the HFH thenmet the staff of each Primary Health Centre (PHC) and
The enthusiasm of the VHNs is unbelievable. When asked
discussed with them the possibility of introducing the POD
what made them accept the responsibility and involve
component in their field area. List of cases treated before
themselves in the programme their stock response is, "We
integration was not available. Initial list of cases who had
never knew that we could bring so much difference to the
been managed by the HFH before integration was handed
lives of these people. They also did not know that such
over to the PHCs. Patients with disability were identified
simple procedures could reduce their suffering and give
from the list by the Village Health Nurses (VHN) accompanied
meaning to their lives. The benefits from our efforts are
by the project field worker. Training (2003) was arranged
first at the PHC and then at each Subcentre. All the MedicalOfficers were trained to manage leprosy and its complications.
The project in collaboration with the DLO has initiated
All the health workers were trained to recognise and refer
holistic service to leprosy affected in 14 PHCs of Pudukottai
reactions and manage patients with disability. The field
district and 17 PHCs of Trichy district. The total population
staff from HFH demonstrated the benefits of selfcare to the
covered is 659168 and 473839 in Trichy and Pudukottai
patients and workers. Monthly combined field visits by the
respectively. In the year 2005 a total of 68 cases (29 MB)
VHN and project worker was arranged. Gradually the VHNs
were detected in these PHCs out of which 26 were referred
were convinced about the immense benefits in the
by VHNs, 4 by General practitioners and 27 reported
intervention. After 3 to 5 months of combined field visits,
voluntarily. On verification of cases wrong diagnosis was
on-the-job training and guidance the VHNs were happy
found to be 4%. There was no reregistration. The PHCs
enough to carry out the activity on their own. When the
diagnosed and treated 7 cases of reaction (2 ENL) and
VHNs and the former vertical staff realised the intentions
3 cases were referred to the NGO project because of
of HFH and saw the benefit to patients, their initial reluctance
complications. The PHCs referred 10 cases with deformity
was replaced by total committed involvement.
for reconstructive surgery. Total number of VHNs in the31 PHCs is 174 of whom 159 are actively involved in
Patients were contacted once a month by the VHNs to
leprosy control including prevention of disability. The total
monitor the status. If there was any complication the patient
number of patients with disability in the 176 subcentres
was immediately referred to the PHC or HFH depending
covered by these VHNs is 427 (33 patients with plantar
on the severity. The VHNs were helped in their work by
anaesthesia, 236 with disabilities including plantar ulcers,
former leprosy staff (paramedical workers). Patients with
158 with disabilities without plantar ulcers). Of these
disability were not issued any gauze or cotton or antiseptic
427 patients 303 were identified by the VHNs. Of the
cream to avoid dependency. Selfcare with available materials
427 patients 363 are found to practice selfcare. In public health, service is the name the providers give; Not the one desired by those who receive. - Krishnamurthy Every patient is a mirror cracked and dense. We don't see in it what we don't wish to see. - Krishnamurthy
Ms. Devi (name changed) aged 24 years from
Siwan District in Bihar had a patch on her right
upper arm since one and a half years and she went
to a local General Practitioner (GP) who treated
her with Rifampicin (450mg daily), Dapsone
(100 mg daily) and Clofazimine (50 mg daily) with
chalmoogra oil for local application for 2 months
with no response. The patient spent Rs.500 for her
The traditional dai from the village asked the
lady to consult the doctor at the PHC where the
Medical Officer, Dr. Sushil Kumar Singh observed
that the patch was erythematous with definite
sensory deficit. The right ulnar was thickened but
not tender. She was correctly diagnosed as PB
elbow. The patient went to the PHC where a diagnosis of Type 1 reaction
leprosy and treatment was initiated. About two
with ulnar neuritis was made. Prednisolone was started.
weeks after the start of treatment the patch became
The PHC did not have prednisolone. Technical Support Team
raised, red and there was severe pain in her right
Delay in reporting to PHC (lack of awareness?)Inappropriate management of disease by the GPReferral by the traditional dai to the PHCCorrect diagnosis of the disease and its complication by the MO at PHCNon-availability of prednisolone for managing reactionTake complete history from patient- useful for diagnosis, management,community interventions (IEC, training of GPs, etc)Do the sensory test correctly to elicit definite sensory deficitExamine the whole body, examine the nerves before coming to a definitive diagnosis.Every person affected with leprosy is at potential risk of developing deformity.Early diagnosis and prompt treatment saves patients from adverse consequences.
Checklist for supervision of records and reports
Card is complete (all the items are filled)
Contents are correct (through verification from interview of patients)
Correct (through verification from interview of patients)
Availability (previous months of current year and annual for the preceding years)
Correct (through verification from treatment register)
In its response to the letter from ILEP coordinator expressing concern on setting up expected goals
for 2006 GOI vide letter dated 29th December 2005 and signed by Dr. D.M. Thorat, DADG (L),
has given the following explanation.
"It is therefore felt necessary to clarify that the goals indicated above are actually "expected outcome"
by December 2005 and March 2006, results from a well managed quality leprosy programme which
led to declining transmission potential of the diseases during the years. These goals therefore should
not be construed as targets given to the States/UTs. However, female patients should receive equal
opportunity to get diagnosed and treated and true new cases as being emphasized in all the meetings
should not be left out of registration.
There is need for State / District authorities and DTSTs working in field to ensure that operational factors
as being reported by NIHFW conducted LEM exercises, are minimal and in addition the States should
strive to provide quality leprosy diagnostic and treatment services at all health facilities"
We thank the Government for the prompt response and clarification. TB CONTROL PROGRAMME
Why some TB patients do not come for follow-up examination?
Microscopy Centre is not accessible.
MO-PHC/ANM to make alternate arrangements:
Sputum samples collected at patient's residence
Centre (or) sputum smears are prepared and
Microscopy Centre is not functioning.
Ensure that sputum microscopy is done and
results are despatched to concerned PHC in time.
Sputum result is not entered in records at PHC.
MO-PHC to review the sputum result and ensure that
results are entered in patient record with DOT provider;
action is initiated based on the sputum results
Adequate counselling of DOT provider at start of
procedures / does not refer the patient.
Mark dates for follow up in patient record with
Patient is not aware of follow up procedure.
Adequate counselling of patient at start of treatment by
Patient is not aware of need for follow up
Sputum cups should be supplied along with RNTCP
medicine pack. DOT provider and patient should know
the procedure; Patient should collect early morning
sputum sample and report to Microscopy Centre where
spot sample would be collected. Two samples could be
given on a single visit to Microscopy Centre.
Periodic visits to patients and DOT providers by any of
the health staff (MO / MPHS / ANM / STS).
STS to check follow up examinations done at MC /
Sensory test for identifying nerve dysfunction
http://www.medscape.com/viewarticle/807694_printEye Therapy Has It Over Antidepressant for PTSDDeborah BrauserEDINBURGH, Scotland — Eye movement desensitization and reprocessing (EMDR) may be a more efficacious treatment for patientswith posttraumatic stress disorder (PTSD) than antidepressant medication, new research suggests. A smal , randomized trial of male survivors of the ongoing war in
EL VISADO PARA LOS ANTIPSICÓTICOS ATÍPICOS ES INACEPTABLE Las alteraciones de conducta en el Alzheimer. Tratamiento farmacológico Los síntomas psicológicos y conductuales asociados a demencia (SPCD) son frecuentes entre los pacientes que padecen esta enfermedad. Existe suficiente evidencia que indica que estas alteraciones tienen una prevalencia en torno al 60-80 % y un riesgo de padecerlas

 Vol. 14 - No. 1
Vol. 14 - No. 1 Dr. P. KRISHNAMURTHY
Dr. P. KRISHNAMURTHY
 leprosy-affected persons at Medical College hospital inPatna and Dharbhanga in Bihar through the coordinated
effort of Government and Damien Foundation India Trust(DFIT) is indeed a laudable initiative. Surgeons and
physiotherapists in these two centres were identified by theGovernment and trained by the visiting surgeon and
physiotherapist from Damien Foundation India Trust. A
set of surgical instruments was provided. Cases requiringsurgery were continuously fed by the District TechnicalSupport Team through the District Leprosy Officer. Following
Finally, all the health facilities in the State should be provided
3 to 4 supervisory training visits by the visiting surgeon and
with the list of referral centres managing reactions or
physiotherapist the staff in the two centres are able to
disabilities or reconstructive surgery so that patients needing
manage patients on their own. Effort should be made to
specialised care could be referred to these centres for
establish at least one such centre in every State preferably
in a Government institution for the sake of sustainability.
leprosy-affected persons at Medical College hospital inPatna and Dharbhanga in Bihar through the coordinated
effort of Government and Damien Foundation India Trust(DFIT) is indeed a laudable initiative. Surgeons and
physiotherapists in these two centres were identified by theGovernment and trained by the visiting surgeon and
physiotherapist from Damien Foundation India Trust. A
set of surgical instruments was provided. Cases requiringsurgery were continuously fed by the District TechnicalSupport Team through the District Leprosy Officer. Following
Finally, all the health facilities in the State should be provided
3 to 4 supervisory training visits by the visiting surgeon and
with the list of referral centres managing reactions or
physiotherapist the staff in the two centres are able to
disabilities or reconstructive surgery so that patients needing
manage patients on their own. Effort should be made to
specialised care could be referred to these centres for
establish at least one such centre in every State preferably
in a Government institution for the sake of sustainability.
 In spite of that POD was not implemented in the districts.
In spite of that POD was not implemented in the districts. Every patient is a mirror cracked and dense.
Every patient is a mirror cracked and dense.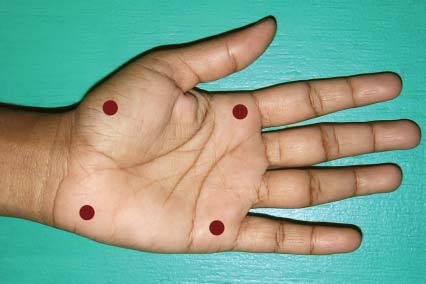
 Sensory test for identifying nerve dysfunction
Sensory test for identifying nerve dysfunction