L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Cineducation.net
Acute Kidney Injury After Cardiac Angiography and Exposure to Iodinated Contrast Media
Panupong Lisawat, MD; Neil Ybanez, MD; and Richard J. Solomon, MD
A 75-year-old female patient with a history of chronic The diagnosis of ST-segment elevation myocardial infarction
kidney disease stage IV, type 2 diabetes mellitus, hyperten-
prompted the initiation of an emergent cardiac catheteriza-
sion and dyslipidemia presented to an outside hospital with a tion. She underwent revascularization with drug-eluting stents. 3-day history of substernal chest pain that radiated to her jaw During the procedure, 100 ml of low osmolar contrast (Isovue and the left side of her back. An electrocardiogram showed 370, Bracco Diagnostics Inc., Princeton, NJ) was used. She was a slight ST elevation in the anterior leads, so she was subse-
stable post-procedure. A nephrology consult was requested to
quently transferred to our hospital. Before transfer, she re-
help manage a potential contrast-induced acute kidney injury.
ceived ticagrelor, aspirin and heparin.
Post catheterization, the patient appeared to be slightly
Her medications before the transfer included losartan, hy-
volume overloaded with bibasilar rales and bilateral 2+ lower
drochlorothiazide, simvastatin, acetylsalicylic acid and insu-
extremity edema. She received 1 dose of intravenous furose-
lin. On admission to our hospital, she was awake and alert, mide post-procedure and produced more than 1 L of urine with a blood pressure of 160/77, a heart rate of 82, and an output. The patient was otherwise stable hemodynamically, oxygen saturation of 97% on room air.
with a minimal supplemental oxygen requirement. Losartan
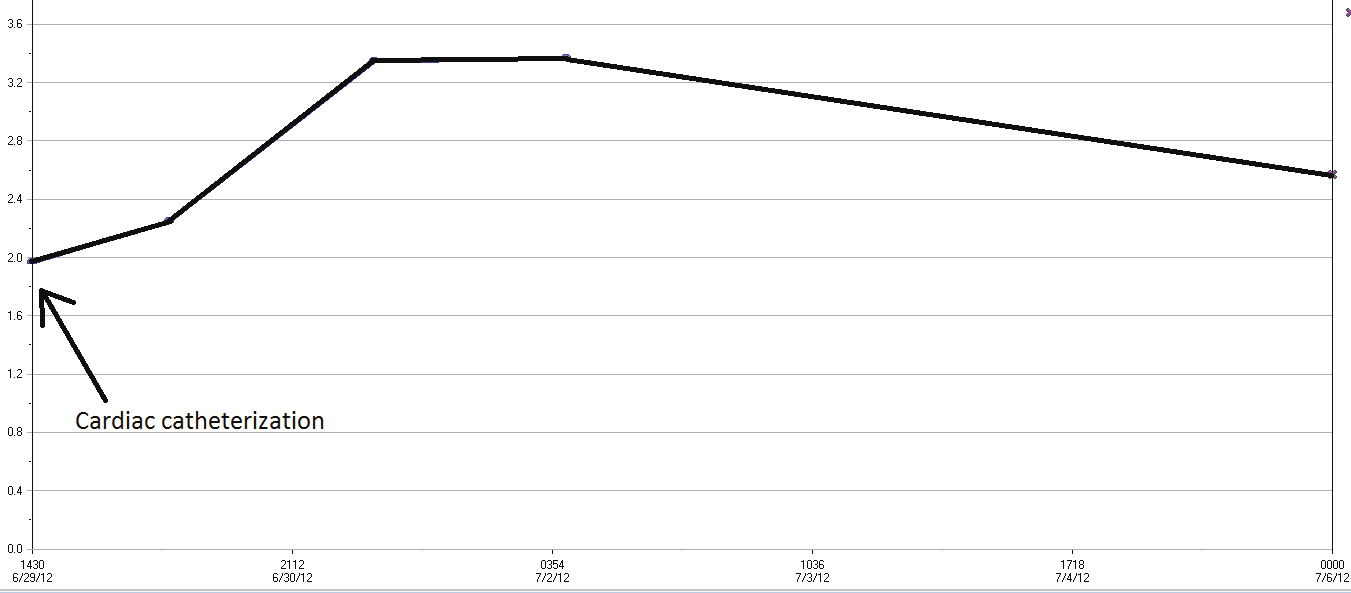
She was found to have a serum creatinine of 1.96 (baseline and hydrochlorothiazide were held.
1.9-2.5 over the past year) that correlated with an eGFR of
Eighteen hours after percutaneous coronary intervention
25 ml/min. Her sodium and potassium concentrations were (PCI), her serum creatinine was 2.24 mg/dl; it had increased to 138 mEq/l and 4.2 mEq/l respectively. Her troponin I was 1.6. 3.34mg/dl at 42 hours. Her urine output decreased from 2900
ml in the first day of admission to 300 ml in the next day.
Furosemide 40 mg oral 2 times daily was started on day 2
From Fletcher Allen Health Care, Burlington, VT. Address for correspondence:
of admission, but the patient had no increase in urine output.
Richard Solomon, MD, Director, Division of Nephrology, Fletcher Allen Health
Care, Burlington, VT, 05401. Email: richard.solomon@vtmednet.org. Disclosures: Dr. Solomon is a consultant/advisor to Bracco Diagnostics, Inc., PLC Med, Inc., and
Her serum creatinine peaked at 65 hours post-PCI at 3.36 mg/
MDSci Inc. He receives honoraria from Guerbet and research grants from REATA
dl (Figure 1). Clinically, the patient was hemodynamically stable.
Pharmaceuticals, Novartis, MDSci, Inc., and Medtronic.
The patient was discharged on the same day on a low-sodium diet. A follow-up serum creatinine 4 days later was 2.56 mg/dl. Discussion Consequences of CIAKI
This patient represents a classic example of acute kidney inju-
CIAKI is a specific form of injury to the kidney. Evidence
ry that occurred after cardiac angiography and exposure to iodin-
that acute kidney injury of any etiology leads to an acceler-
ated contrast media. Contrast media are water-soluble organic ated loss of kidney function is just beginning to be appreci-molecules that contain iodine and are excreted almost entirely by ated.6 Both small prospective studies7 and retrospective analyses the kidneys, with a half-life measured in a few hours.
of large databases8 indicate that patients who develop CIAKI
First described in 1954, what we now call contrast-induced progress to worse kidney function over the ensuing years com-
acute kidney injury (CIAKI) is defined by a change in serum pared to those without CIAKI. creatinine that follows a characteristic course (see Figure 1).1
In the short-term, CIAKI increases hospital length of stay,
Creatinine begins to rise usually within 24 hours of exposure in-hospital mortality and overall cardiovascular mortality over and peaks on day 3 or 4 before slowly returning to or close to the following 5 years.9 Are these adverse events caused by the the baseline value over the next 7-10 days. Other explanations CIAKI, or are patients who develop CIAKI already destined for a change in creatinine must first be excluded.
for worse outcomes because of their comorbid conditions and
The threshold increase required for a definition of CIAKI the burdens of risk factors? The answer to this question is of
varies in the literature from a relative increase of 25% to an abso-
great importance and the subject of ongoing study.
lute increase of 0.5 mg/dL. These definitions produce different incidences of CIAKI in the same population, making it difficult Prevention of CIAKI to compare studies on prevention. Among patients undergoing
Because the administration of contrast is predictable and
cardiac angiography, the incidence of CIAKI is ~5% but can the consequences of CIAKI are significant, efforts to prevent increase to more than 50% in some high-risk patients. In pa-
this form of kidney injury are indicated. Knowledge of the
tients undergoing contrast-enhanced computed tomography ex-
pathophysiology of CIAKI has led to a number of strategies.
ams, the incidence even in patients with chronic kidney disease
The first step is identifying which patients are most likely
appears less often and depends on the setting (inpatient versus to suffer CIAKI. Patients with decreased kidney function be-outpatient) and whether severe renal dysfunction is present.2
fore contrast exposure are at higher risk because each remaining
The Acute Kidney Injury Network (AKIN) group has pro-
nephron must excrete a greater load of the contrast, thus in-
posed a new definition of acute kidney injury as an absolute creasing the potential for toxicity. Any condition that compro-0.3 mg/dL increase in creatinine within a 48-hour period, or a mises renal blood flow at baseline will further increase the risk. decrease in urine output to less than 0.5 mg/kg/h and sustained For example, patients with congestive heart failure, volume for at least 6 hours despite corrective measures.3 This defini-
depletion, current NSAID use and a limited ability to gener-
tion is just beginning to gain acceptance in the cardiology and ate nitric oxide (such as patients with diabetes) are all at some radiology literature.
increased risk. Patients with hemodynamic instability at the time of angiography - particularly those requiring supportive
Pathophysiology
measures, such as the use of pressors or an intra-aortic balloon
Contrast media are nephrotoxic to the kidneys through at pump - are at increased risk. Finally, the more contrast agent
least two mechanisms. First, all contrast media decrease blood used, the greater the CIAKI risk. A scoring system to calculate flow to the kidney, particularly in the medullary portion of the not only the incidence of CIAKI but also the need for renal kidney. Studies of isolated descending vasa recta, the main ves-
replacement therapy has been in use for a number of years.10
sels supplying oxygen to the tubules in the medulla, indicate
Once a high-risk patient has been identified, the next
that contrast media cause vasoconstriction mediated by the step is to minimize the modifiable risk factors. Volume-de-generation of reactive oxygen species and a decrease in avail-
pleting agents (diuretics) and NSAIDs should be held and
ability of nitric oxide.4 This causes an ischemic injury in this intravenous fluid administered. Although some controver-portion of the kidney. Additional mechanisms of injury occur sies exist regarding the type, amount, and duration of IV through direct toxicity to the cells lining the renal tubules. This fluid, most recommendations include normal saline at 1 ml/injury also generates reactive oxygen species and proapoptotic kg/h for 4-6 hours before and 12 hours after cardiac an-stimuli, leading to loss of cell viability.5
giography. The amount can be increased to 3 ml/kg as a
The contrast effects on vasa recta and tubule cells result in a de-
bolus for urgent/emergency cases, and modified to 1.5 ml/
crease in glomerular filtration rate (GFR) and, thus, a rise in creati-
kg bolus in the presence of the symptoms of congestive heart
nine. The toxicity of contrast is not directly on the glomerulus, and failure. The use of IV fluid has now been incorporated into the decrease in filtration is a response to the downstream damage the latest guideline from the American Heart Association/to the tubule through a process called tubuloglomerular feedback American College of Cardiology (AHA/ACC).11 However, (TGF). Although the change in GFR occurs early in the course of despite the use of IV fluid, the incidence of CIAKI in high-CIAKI, it takes days for enough creatinine to be retained in the risk patients remains ~10%. body to reach the threshold for a diagnosis of CIAKI. Newer in-
The central pathophysiologic role of ischemia and the
jury markers analogous to a renal troponin, such as NGAL, KIM-
generation of reactive oxygen species have led to the use
1, and IL-18, will hopefully permit earlier diagnosis of this injury.
of antioxidant therapy as a strategy to prevent CIAKI.
N-acetylcysteine (NAC) is a scavenger of reactive oxygen medium is used, every effort should be make to minimize species and a precursor of glutathione, a natural antioxidant. the amount of contrast administered. Although initial studies suggested a preventive effect,12 sub-sequent prospective randomized trials and summary meta-
analyses13 have diminished enthusiasm for this approach. As
CIAKI reflects injury to the kidney and risk for cardiovascu-
with any therapy, dose becomes critical, and a soon-to-begin lar events, mortality, subsequent progression of chronic kidney trial will use a high dose administered for a longer duration disease, and the need for dialysis. Patients at greatest risk can be (NCT01467466).
identified in advance, and most institutions take steps to mini-
The use of isotonic sodium bicarbonate as the IV infu-
mize the risk, such as using isotonic fluid administration and
sion fluid instead of sodium chloride was proposed based antioxidants, and minimizing use of contrast. Specific protocols up the importance of acid pH in the generation of some to risk stratify and treat patients undergoing contrast administra- reactive oxygen species. Because urine is generally acidic, tion have been shown to improve patient outcomes.23,24 New and administration of sodium bicarbonate to alkalinize the urine novel approaches to prevention continue to be investigated. was initially found to reduce the incidence of CIAKI.14 As with NAC, subsequent studies have reported mixed results, References although meta-analyses15 still suggest a benefit. One mul-
1. Bartels ED, Brun GC, Gammeltoft A, Gjørup PA. Acute anuria following intravenous
ticenter trial using a higher dose of bicarbonate to ensure
pyelography in a patient with myelomatosis. Acta Med Scand. 1954;150(4):297-302.
2. Weisbord SD, Mor MK, Resnick AL, et al. Incidence and outcomes of con-
urinary alkalinization is ongoing (NCT00930436).
trast-induced AKI following computed tomography. Clin J Am Soc Nephrol.
A variety of approaches to inducing vasodilation in the
kidney have met with limited success. Atrial natriuretic pep-
3. Mehta RL, Kellum JA, Shah SV, et al; Acute Kidney Injury Network. Acute Kidney
Injury Network: report of an initiative to improve outcomes in acute kidney injury.
tide, dopamine receptor agonists, prostaglandin E2, theoph-
ylline, endothelin antagonists and adenosine antagonist have 4. Sendeski M, Patzak A, Persson PB. Constriction of the vasa recta, the vessels sup-all been studied in man or animal models, but have yet to gain
plying the area at risk for acute kidney injury, by four different iodinated contrast media, evaluating ionic, nonionic, monomeric and dimeric agents. Invest Radiol.
Novel approaches to preventing CIAKI have included extra-
5. Romano G, Briguori C, Quintavalle C, et al. Contrast agents and renal cell apoptosis.
corporeal cooling of the patient, use of a coronary sinus catheter
Eur Heart J. 2008;29(20):2569-2576.
6. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney in-
to remove contrast before it reaches the systemic circulation, and
jury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442-448.
hemodialysis or hemofiltration to remove contrast. The only re-
Goldenberg I, Chonchol M, Guetta V. Reversible acute kidney injury fol-
ported success has been with hemofiltration, in which Ringer's
lowing contrast exposure and the risk of long-term mortality. Am J Nephrol. 2009;29(2):136-144.
lactate (a source of bicarbonate) is given at 1 l/h as an isovolemic 8. James MT, Ghali WA, Knudtson ML, et al; Alberta Provincial Project for Outcome replacement fluid for the ultrafiltrate of plasma that is removed.16
Assessment in Coronary Heart Disease (APPROACH) Investigators. Associations
A recent additional approach has been the induction of a high
between acute kidney injury and cardiovascular and renal outcomes after coronary angiography. Circulation. 2011;123(4):409-416.
urine flow rate (300-800 ml/h) by real-time ml/ml replacement 9. Brown JR, Malenka DJ, DeVries JT, et al; Dartmouth Dynamic Registry Investiga-of urine output after a saline bolus (250 m) and dose of furose-
tors. Transient and persistent renal dysfunction are predictors of survival after per-
mide (0.25 mg/kg). Two large European trials have reported suc-
cutaneous coronary intervention: insights from the Dartmouth Dynamic Registry. Catheter Cardiovasc Interv. 2008;72(3):347-354.
cess with this approach, which presumably dilutes the contrast in 10. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of con-the renal tubule.17,18 A US trial with this device recently got under
trast-induced nephropathy after percutaneous coronary intervention: development
way (NCT01456013). Finally, a recent trial reporting a benefit of
and initial validation. J Am Coll Cardiol. 2004;44(7):1393-1399.
11. Wright RS, Anderson JL, Adams CD, et al. 2011 ACCF/AHA focused update of the
remote ischemic preconditioning requires further confirmation.19
Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation
Finally, the choice of contrast media has been a con-
Myocardial Infarction (updating the 2007 guideline): a report of the American Col-
troversial theme in the study of CIAKI. The first cases of
lege of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American College of Emergency
CIAKI occurred with high osmolar contrast (~1500 mOsm/
Physicians, Society for Cardiovascular Angiography and Interventions, and Society of
kg). When low osmolar contrast (~600-700 mOsm/kg) be-
Thoracic Surgeons. J Am Coll Cardiol. 2011;57(19):1920-1959.
came available, comparative trials found a lower incidence of 12. Tepel M, van der Giet M, Schwarzfeld C, et al. Prevention of radiographic-con-
trast-agent-induced reductions in renal function by acetylcysteine. N Engl J Med.
kidney injury in high-risk patients with the lower osmolar
agents.20 This naturally led to the hypothesis that the osmo-
13. Gonzales DA, Norsworthy KJ, Kern SJ, et al. A meta-analysis of N-acetylcysteine
larity of the contrast determined nephrotoxicity. The more
in contrast-induced nephrotoxicity: unsupervised clustering to resolve heterogeneity. BMC Med. 2007;5:32.
recent availability of iso-osmolar contrast (~290 mOsm/kg) 14. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with and an initial positive comparative trial of iso-osmolar versus
sodium bicarbonate: a randomized controlled trial. JAMA. 2004;291(19):2328-2334.
low osmolar contrast fueled this hypothesis.21 However, sub-
15. Hoste EA, De Waele JJ, Gevaert SA, Uchino S, Kellum JA. Sodium bicarbonate for
prevention of contrast-induced acute kidney injury: a systematic review and meta-
sequent prospective randomized trials have failed to repli-
analysis. Nephrol Dial Transplant. 2010;25(3):747-758.
cate the original findings, and meta-analyses22 also found no 16. Marenzi G, Lauri G, Campodonico J, et al. Comparison of two hemofiltration proto-difference in the incidence of CIAKI between iso-osmolar
cols for prevention of contrast-induced nephropathy in high-risk patients. Am J Med. 2006;119(2):155-162.
and low osmolar contrast. The AHA/ACC 2011 guidelines 17. Marenzi G, Ferrari C, Marana I, et al. Prevention of contrast nephropathy by furo-reflect this lack of difference.11 Regardless of which contrast
semide with matched hydration: the MYTHOS (Induced Diuresis With Matched Hydration Compared to Standard Hydration for Contrast Induced Nephropathy Pre-
vention) trial. JACC Cardiovasc Interv. 2012;5(1):90-97.
Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med.
18. Briguori C, Visconti G, Focaccio A, et al; REMEDIAL II Investigators. Renal Insuf-
ficiency After Contrast Media Administration Trial II (REMEDIAL II): RenalGuard
22. Heinrich MC, Häberle L, Müller V, Bautz W, Uder M. Nephrotoxicity of iso-osmolar
System in high-risk patients for contrast-induced acute kidney injury. Circulation.
iodixanol compared with nonionic low-osmolar contrast media: meta-analysis of ran-
domized controlled trials. Radiology. 2009;250(1):68-86.
19. Er F, Nia AM, Dopp H, et al. Ischemic preconditioning for prevention of contrast
23. Taylor AJ, Hotchkiss D, Morse RW, McCabe J. PREPARED: Preparation for Angiog-
medium-induced nephropathy: randomized pilot RenPro trial (Renal Protection
raphy in Renal Dysfunction: a randomized trial of inpatient vs outpatient hydration
Trial). Circulation. 2012;126(3):296-303.
protocols for cardiac catheterization in mild-to-moderate renal dysfunction. Chest.
20. Barrett BJ, Carlisle EJ. Metaanalysis of the relative nephrotoxicity of high- and low-
osmolality iodinated contrast media. Radiology. 1993;188(1):171-178.
24. Marenzi G, Lauri G, Campodonico J, et al. Comparison of two hemofiltration proto-
21. Aspelin P, Aubry P, Fransson SG, et al; Nephrotoxicity in High-Risk Patients Study
cols for prevention of contrast-induced nephropathy in high-risk patients. Am J Med.
of Iso-Osmolar and Low-Osmolar Non-Ionic Contrast Media Study Investigators.
All rights reserved. Reproduction in whole or in part prohibited.
SENSORY ACTIONS OF ANTIMUSCARINICSFINNEY et al. Antimuscarinic drugs in detrusor overactivity and the overactive bladder syndrome: motor or sensory actions? STEVEN M. FINNEY, KARL-ERIK ANDERSSON*, JAMES I. GILLESPIE† and LAURENCE H. STEWART Western General Hospital, Edinburgh, UK, *Department of Clinical and Experimental, Pharmacology, Lund University Hospital, Sweden, and †The Urop
Charlene Kramer Email:chkramer2002@yahoo.com Cell #:989-553-4441 Career Portfolio:www.chkramer.net SUMMARY OF QUALIFICATIONS Experienced in support staffing and management in many fast paced industries such as construction, marketing and healthcare just to name a few. A self-motivated individual, who is reliable and eager to accept new and challenging roles and responsibilities as needed
 Acute Kidney Injury After Cardiac Angiography and
Acute Kidney Injury After Cardiac Angiography and