Real-time Prescription Surveillance and its Application toMonitoring Seasonal Influenza Activity in Japan
Tamie Sugawara1, PhD; Yasushi Ohkusa1, PhD; Yoko Ibuka2, PhD; Hirokazu Kawanohara3, BS; Kiyosu Taniguchi1,
1National Institute of Infectious Diseases, Infectious Disease Surveillance Center, Tokyo, Japan2Hitotsubashi University, Tokyo, Japan3EM Systems Co., Ltd, Tokyo, Japan
Corresponding Author: Tamie Sugawara, PhD National Institute of Infectious Diseases Infectious Disease Surveillance Center 1-23-1Toyama Shinjuku Tokyo, 162-8640 Japan Phone: 81 3 5285 1111 Fax: 81 3 5285 1129 Email: Background: Real-time surveillance is fundamental for effective control of disease outbreaks, but the official sentinel surveillance in Japan collects information related to disease activity only weekly and updates it with a 1-week time lag. Objective: To report on a prescription surveillance system using electronic records related to prescription drugs that was started in 2008 in Japan, and to evaluate the surveillance system for monitoring influenza activity during the 2009-2010 and 2010-2011 influenza seasons. Methods: We developed an automatic surveillance system using electronic records of prescription drug purchases collected from 5275 pharmacies through the application service provider's medical claims service. We then applied the system to monitoring influenza activity during the 2009-2010 and 2010-2011 influenza seasons. The surveillance system collected information related to drugs and patients directly and automatically from the electronic prescription record system, and estimated the number of influenza cases based on the number of prescriptions of anti-influenza virus medication. Then it shared the information related to influenza activity through the Internet with the public on a daily basis. Results: During the 2009-2010 influenza season, the number of influenza patients estimated by the prescription surveillance system between the 28th week of 2009 and the 12th week of 2010 was 9,234,289. In the 2010-2011 influenza season, the number of influenza patients between the 36th week of 2010 and the 12th week of 2011 was 7,153,437. The estimated number of influenza cases was highly correlated with that predicted by the official sentinel surveillance (r =.992, P <.001 for 2009-2010; r =.972, P <.001 for 2010-2011), indicating that the prescription surveillance system produced a good approximation of activity patterns. Conclusions: Our prescription surveillance system presents great potential for monitoring influenza activity and for providing early detection of infectious disease outbreaks. (J Med Internet Res 2012;14(1):e14) Â Â KEYWORDS
Surveillance; influenza; real-time surveillance; prescriptions; pharmacy; anti-influenza virus; automatic surveillance; earlyresponse
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.1
(page number not for citation purposes)
Web-based surveillance, tracks the rate of influenza using querylogs In addition to monitoring disease activities, syndromic
In Japan, the official sentinel surveillance reports the number
surveillance helps monitor bioterrorism-related disease or
of influenza patients per health care provider after collecting
health consequences of natural events ].
information from approximately 5000 clinics and hospitals. The
Real-time information related to influenza activity is
intensity of influenza activity is assessed according to the
number of influenza patients per clinic or hospital. Influenza is
countermeasures against a sudden increase of influenza activity.
regarded as highly active if the ratio exceeds 1. In 2009, the
Therefore, daily updates of influenza activity are indispensable
number of patients per clinic or hospital approached 1 in the
for improved understanding and control of an influenza
32nd week, earlier than in any of the preceding 10 years, mainly
epidemic. We developed an automatic real-time prescription
because of the influenza pandemic A (H1N1), which started in
surveillance system with the collaboration of EM Systems Co.
April 2009 Accordingly, the vast majority of the reported
Ltd. (Tokyo, Japan) to provide timely information related to a
cases were H1N1 novel influenza []. The number of influenza
disease outbreak. We applied the surveillance system to monitor
patients per health care provider declined below 1 in the 13th
influenza activity during the 2009-2010 and 2010-2011
week of 2010. The total number of weeks during which
influenza seasons to examine the magnitude and trajectory of
influenza was highly active was 29, a longer active period than
an outbreak more closely and to share that information with
in any of the prior 10 years. In 2010, the reported number of
public health authorities, as well as participating pharmacies.
influenza patients per clinic or hospital exceeded 1 in the 50thweek []; a second peak week was detected in March 2011.
We used prescription drug purchase data for surveillance of
Because of these irregular patterns of influenza activity, it is
influenza activity for three reasons. First, prescribing
necessary that both policy makers and clinicians follow
anti-influenza drugs such as oseltamivir or zanamivir is a
influenza activity closely to implement effective control of an
common clinical practice for diagnosed influenza cases in Japan.
influenza outbreak throughout the year.
Japan has the highest annual level of oseltamivir usage in theworld [Therefore, prescription drugs can serve as a good
Syndromic surveillance is a useful tool for seasonal influenza
indicator of the overall number of influenza patients. Physicians
monitoring []. In Japan, the official sentinel surveillance of
often perform rapid influenza diagnostic tests on patients who
infectious diseases is implemented by the National Institute of
have a fever or report other influenza-like symptoms. If the test
Infectious Diseases. It reports the estimated number of influenza
result is positive or, alternatively, if the physician clinically
patients weekly as the Infectious Diseases Weekly Report
diagnoses influenza even when the test result is negative, then
The official sentinel surveillance collects the number of
anti-influenza drugs are often prescribed. This contrasts to
influenza cases from approximately 5000 hospitals and clinics
practices in some other developed countries, where
all over the country and then estimates the number of influenza
anti-influenza drugs are recommended for those who are at high
patients based on the reported cases []. The entire process of
risk [or who have severe conditions from influenza
collecting information from health care providers, estimating
infections []. In such circumstances, surveillance of
the number of clinical influenza cases, and reporting them to
prescriptions of anti-influenza drugs would trace influenza
the public usually takes 7-10 days. Furthermore, the cases are
reported by health care providers as a weekly aggregate number. Some diseases spread rapidly, and the weekly aggregates might
Second, many pharmacies have adopted the electronic
not provide sufficiently detailed information reflecting the
prescription record system (EPRS), which enables automatic,
complete character of disease activity. In addition, the official
continuous, and constant information collection, and real-time
sentinel surveillance updates influenza activity less frequently
analysis of prescriptions and patients. In Japan, the utilization
during major holidays. In Japan, seasonal influenza activity
rate of the EPRS among pharmacies was 99.0% in 2009 ].
usually starts to become active during the New Year holidays.
Japan also has a high rate of outpatient or office-based clinician
Constant monitoring and reporting of activity during that period
visits in cases where people feel ill [partly because of the
universal health insurance system. Therefore, one might inferthat the number of influenza patients collected through the EPRS
Syndromic surveillance is in widespread use for monitoring
would closely approximate the number of symptomatic influenza
diseases, but usage of prescription drug sales as a source of
information is fairly limited. In the United States, the mostcommon source of syndromic surveillance reported by health
Third, in contrast to the United States or Taiwan ], in Japan
officials is emergency department visits (84%), followed by
electronic medical record (EMR) systems are not yet well
outpatient clinic visits (49%) and over-the-counter medication
established. In the United States, surveillance for influenza
sales (44%); less than 10% of health departments reported
activity is based on data on outpatient visits along with data
prescription medications as a source In the context of
related to sales of over-the-counter drugs, school absenteeism,
influenza, emergency department surveillance is used to monitor
and ambulatory care encounters ,Surveillance for
the impact of influenza by age For more rapid feedback,
influenza activity using the EMR has been intensively discussed
the Web recently has become a powerful tool for syndromic
and widely applied ]. By contrast, the Survey of Medical
surveillance For example, health surveillance using a
Institutions by the Ministry of Health, Labour and Welfare in
Web-based self-reporting daily questionnaire is applied to
Japan showed that the share of health care providers using EMRs
monitor influenza activities ]. Google Flu Trends, a
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.2
(page number not for citation purposes)
was just over 10% in 2008, or 948 hospitals (10.8% of all
service provider, data related to prescriptions from all
hospitals) and 12,939 clinics (13.1% of all clinics) [
participating pharmacies were collected and deposited in a singleserver, making the data collection secure, efficient, and nearly
We developed the surveillance system to collect the number of
cost-free. Medications covered by the surveillance system
prescriptions together with patients' characteristics from the
included drugs for relief of fever and pain, drugs for common
EPRS automatically, to analyze the data simultaneously to
colds, antibiotics, and antiviral drugs including anti-influenza
estimate the number of influenza cases, and then to provide
virus drugs and antivaricella-zoster virus drugs. The current
real-time information of influenza activity to health care
study specifically addressed prescriptions for anti-influenza
providers and policy makers. The system was tested for a limited
virus medication. The neuraminidase inhibitors oseltamivir,
time at the G8 Summit meeting in Toyako, Hokkaido in July
zanamivir, and laninamivir were included, but amantadine was
2008 for 1 month ]. The present report summarizes details
excluded because it is not commonly prescribed for influenza
of our prescription surveillance system and presents an
evaluation of its performance in the first two influenza seasons,those of 2009-2010 and 2010-2011, since the start of the
The original prescriptions contain information related to
nationwide operation of the system. The evaluation of
patients' sociodemographic and social security information, as
surveillance performance, particularly outbreak detection
well as the health care providers' information. The automatic
performance, is challenging and few studies conduct such
surveillance system aggregated the number of prescriptions for
analyses ]. A study showed that weekly variation in visits
each type of drug and provided tabulations by age and by
for lower respiratory tract infections approximated the national
geography at both national and prefectural levels. The number
mortality data for pneumonia and influenza [Similarly, our
of influenza patients was then estimated from the aggregated
retrospective evaluation analyzed how closely the estimates of
number of prescriptions for anti-influenza drugs by adjusting
influenza cases followed the trajectory of influenza epidemics
the number of prescriptions for anti-influenza drugs with the
proportion of participating pharmacies and of prescriptionspurchased through pharmacies. The analysis and estimation
were conducted overnight and the report of the analysis wassent automatically at 7:00 AM on the next day to the registered
Prescription Surveillance
recipients, including participating pharmacies and public health
We started collecting and analyzing data related to prescriptions
authorities. In addition, figures showing the number of
automatically through the application service provider of the
prescriptions for each type of drug and of the estimated number
EPRS in April 2009 [As of March 2011, the
of patients were created and posted on the website for public
number of participating pharmacies was 5275. In the application
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.3
(page number not for citation purposes)Figure 1. Prescription surveillance. Pharmacies A-D use the application service provider's (ASP) medical claims service. All data are stored in a central database. The surveillance system automatically counts oseltamivir, zanamivir, and laninamivir prescriptions at the data center. The information is analyzed using multiple regression models. The results are presented as figures and tables and feedback to participating pharmacies as well as public health authorities.
prefecture was calculated and reported publicly ]. The
Performance Evaluation
number of influenza patients in Gifu Prefecture was surveyed
We evaluated our surveillance system from two perspectives
during November 16-22, 2009 by the local public health
for the 2009-2010 and 2010-2011 influenza seasons. First, we
authority as a response to the A/H1N1 influenza pandemic. A
compared the estimated number of influenza patients with the
survey questionnaire asking for the number of influenza patients
estimates provided by the official sentinel surveillance []. The
who visited health care providers was sent to all hospitals and
official sentinel surveillance estimates the number of influenza
clinics located within the prefecture (total of 1677 health
patients based on the number of influenza patients reported by
providers); 1033 providers responded to the survey (response
5000 health care providers, including 3000 pediatricians, in
Japan. We chose the evaluation period to include the periodwhen influenza activity was high for the 2009-2010 influenza
The Internal Review Board at the National Institute of Infectious
season. The epidemiological threshold of seasonal influenza
Diseases approved the current study (approval number 57,
activity is determined by the number of influenza patients per
"Development and application of real-time surveillance system
hospital or clinic. If the ratio is equal to or greater than 1 based
to monitor syndromic and symptomatic cases using electronic
on the official sentinel surveillance, activity is high by the
definition that is accepted and widely used throughout Japan
[]. This corresponds to the period between the 28th week of2009 (the week starting on July 6, 2009) and the 12th week of
For the 2009-2010 influenza season, the total number of
2010 (the week starting on March 21, 2010) for the 2009-2010
influenza patients estimated by the prescription surveillance
influenza season. For the 2010-2011 season, the performance
system between the 28th week of 2009 and the 12th week of
was evaluated between the 36th week of 2010 (the week starting
2010 was 9,234,289 ). The largest number of influenza
on September 6, 2010) and the 12th week of 2011 (the week
patients, 234,519, was reported on November 24, 2009. For the
starting on March 21, 2011). Second, for the 2009-2010
2010-2011 influenza season, the number of influenza patients
influenza season, we also compared our estimates with the
between the 36th week of 2010 and the 12th week of 2011 was
number of influenza patients estimated by the Gifu Medical
7,153,437 The largest number of influenza patients,
Association, where the total number of influenza patients in the
230,288, was reported on January 24, 2011. The official sentinel
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.4
(page number not for citation purposes)
surveillance estimated the total number of patients for the same
(95% confidence interval 13,350,000-14,010,000) for the
2010-2011 influenza seasons [indicating that the sentinel
20,460,000-20,860,000) for the 2009-2010 and 13,680,000
estimates were approximately double our estimates. Table 1. Number of influenza cases estimated by the prescription surveillance, the official sentinel surveillance, and the Gifu Medical Association in
Gifu Prefecture, 2009-2010 and 2010-2011 influenza seasonsa
Estimate by the prescription surveillance
Estimate by the official sentinel surveillance
Adjusted estimation by the survey in Gifu Prefecture
a Sources: the official sentinel surveillance []; Kawai et al b Adjusted estimation by the survey in Gifu Prefecture is shown only for the 2009-2010 influenza season because the data are available only for thatyear.
Pearson correlation coefficient (r) of time-series data on
The estimated number of influenza cases in the 2009-2010
influenza patients between our estimates and the official sentinel
influenza season was also compared with that ascertained from
estimate was.992 (P <.001) for the 2009-2010 influenza
the survey of the number of influenza patients at all clinics and
season, and.972 (P <.001) for the 2010-2011 influenza season
hospitals conducted in Gifu Prefecture. The estimated number
(see ). A similar analysis was conducted at the
from the survey collection in the prefecture based on the
prefecture level. The correlation was.950 or greater in 33
prescription surveillance was 127,568, whereas the number of
prefectures,.900-.949 in 5 prefectures, and.770-.899 in 8
influenza cases reported by the survey conducted by Gifu
prefectures. The correlation was the lowest in Akita Prefecture
Medical Association was 132,474. The official sentinel
surveillance estimated the number as 277,890. Figure 2. Number of influenza cases, 2009-2011, estimated by the prescription surveillance and reported by the official sentinel surveillance. The estimated number of influenza cases by prescription surveillance was calculated based on the number of oseltamivir, zanamivir, and laninamivir prescriptions adjusted by the proportion of participating pharmacies and extramural dispensing percentage. See text for details. The reported number by the official sentinel surveillance shows the number of influenza patients per clinic or hospital, calculated with the reported number of influenza patients from 5000 sentinel clinics and hospitals.
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.5
(page number not for citation purposes)
is covered by the sentinel surveillance, continuous monitoringof influenza activity is necessary to detect outbreaks early in
Our analyses showed that the time-series pattern of influenza
their course. Our automatic prescription surveillance system
activity reported by the prescription surveillance system in the
uses the same standard for detection of a disease outbreak and
first two influenza seasons was highly correlated with the pattern
runs continuously, providing an important complementary role
reported by the official sentinel surveillance, showing that
in support of existing surveillance systems in Japan.
pharmacy surveillance can be a good indicator of influenza
If EMRs were widely kept, then information related to influenza
activity in Japan. Although the estimated number of influenza
patients could be collected even faster and possibly more
patients was double that of the official sentinel surveillance, it
accurately. However, the share of health care providers that
was close to the estimate by Gifu Prefecture, where the total
have adopted the EMR system was slightly above 10%. Under
number of influenza patients was collected in a survey.
such circumstances, purchases of anti-influenza drugs can serve
The significance of our prescription surveillance is threefold.
as an alternative indicator of influenza activity.
First, the syndromic surveillance system collected, analyzed,
Limitations to this study exist. First, the total number of
and reported data related to influenza patients simultaneously.
influenza cases was estimated as almost half of the estimate
Therefore, clinicians and policy makers were able to obtain the
based on the official sentinel surveillance, although it
estimated number of influenza patients of the previous day. This
approximated estimates based on a survey collecting the total
meant that the estimates were available 1 week ahead of those
number of influenza cases in Gifu Prefecture. One reason for
reported by the official sentinel surveillance, enabling
this gap might lie in the choice of health care providers
predictions of influenza activity for the immediately following
participating in the official sentinel surveillance. The sentinel
week. This was particularly important at the outset of a seasonal
health care providers have, on average, a larger number of
epidemic, when the trajectory of a quickly spreading disease
patients than others, potentially resulting in an overestimation
would have changed. Though the Google Flu Trends tool,
of the overall number of influenza patients. Second,
another real-time surveillance, has been shown to perform well
anti-influenza drugs are also prescribed for prophylaxis in
in the United States and European countries ], the results
addition to treatment, which might engender overestimation of
may be sensitive to variations in patients' behavior across
the total number of influenza cases. However, in Japan the
preventive usage of oseltamivir is limited to household members
Second, our prescription surveillance was national and observed
of influenza patients who are 65 years or older or who are
regional variations in influenza activity at the prefecture level,
high-risk individuals ]. Third, the prophylactic usage of
although the precision of surveillance varied somewhat between
anti-influenza drugs for health care providers and for the public
prefectures. This provided helpful information to public health
was most intensive at the beginning of the H1N1 pandemic
services to plan for the allocation of medical, pharmaceutical,
outbreak. We did not include those prescriptions in our
and human resources for influenza control, shifting limited
surveillance data because they were not prescribed through
resources to the most affected regions.
health care providers. Fourth, 60% of the prescriptions werepurchased through pharmacies in 2008. The other prescriptions
Third, our surveillance runs constantly, maintaining the method
were purchased directly through health care providers and were
of counting and estimating influenza cases at all times, and thus
not included in our surveillance [This is still much higher
we were able to obtain the complete trajectory of the influenza
than the rate of adoption of the EMR system in hospitals and
pandemic in the 2009-2010 season. Initially during the
clinics. Fifth, the participation rate of pharmacies is low,
pandemic, the law required hospitals and clinics to report all
particularly in certain areas. If the number of participating
influenza cases, but that practice was terminated on July 24,
pharmacies were increased, then estimating influenza cases
2009, after which activity was tracked only by the official
would be possible even for smaller geographical units.
Despite these limitations, pharmacy surveillance provided an
Our surveillance system also promises great potential for future
approximation of the trend of influenza activity in the first two
application to the early detection of an infectious disease
influenza seasons after the start of its nationwide operation. It
outbreak or bioterrorism attack, which could happen potentially
provided both clinicians and policy makers with helpful
anywhere at any time. When we started operating a prescription
real-time information related to influenza activity. Our pharmacy
surveillance system in 2009, all other surveillance systems
surveillance system has great potential for detection as well as
running in Japan covered only specific regions of the country
for monitoring of infectious disease outbreaks in the population
for practical reasons ]. Furthermore, because influenza
and in cases of significant political or cultural events.
outbreaks do not necessarily occur during winter, the time that
Acknowledgments
This research was financially supported by a Health and Labour Sciences Research Grant from the Ministry of Health, Labourand Wealth, "Research for practical application of early detection system for health risk," headed by the second author, Dr YasushiOhkusa. Dr Yoko Ibuka received a grant from the Abe Fellowship Program administered by the Social Science Research Council
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.6
(page number not for citation purposes)
and the American Council of Learned Societies in cooperation with and with funds provided by the Japan Foundation Center forGlobal Partnership. Conflicts of Interest References 1.
Shimada T, Gu Y, Kamiya H, Komiya N, Odaira F, Sunagawa T, et al. Epidemiology of influenza A(H1N1)v virus infectionin Japan, May-June 2009. Euro Surveill 2009 Jun 18;14(24) [Medline:
National Institute of Infectious Diseases. 2011. Infectious Diseases Weekly Report: Trend Graph [in Japanese] [accessed 2011-06-30]
Buehler JW, Sonricker A, Paladini M, Sope P, Mostashar F. Syndromic surveillance practice in the United States: findingsfrom a survey of state, territorial, and selected local health departments. Adv Dis Surveill 2008;6(3).
Taniguchi K, Hashimoto S, Kawado M, Murakami Y, Izumida M, Ohta A, et al. Overview of infectious disease surveillancesystem in Japan, 1999-2005. J Epidemiol 2007 Dec;17 Suppl:S3-13 ]
Olson DR, Heffernan RT, Paladini M, Konty K, Weiss D, Mostashari F. Monitoring the impact of influenza by age:emergency department fever and respiratory complaint surveillance in New York City. PLoS Med 2007 Aug;4(8):e247[] [Medline:
Brownstein JS, Freifeld CC, Reis BY, Mandl KD. Surveillance Sans Frontières: Internet-based emerging infectious diseaseintelligence and the HealthMap project. PLoS Med 2008 Jul 8;5(7):e151 ] [doi:]
Sugiura H, Ohkusa Y, Akahane M, Sano T, Okabe N, Imamura T. Development of a web-based survey for monitoringdaily health and its application in an epidemiological survey. J Med Internet Res 2011;13(3):e66 [doi:]
Ginsberg J, Mohebbi MH, Patel RS, Brammer L, Smolinski MS, Brilliant L. Detecting influenza epidemics using searchengine query data. Nature 2009 Feb 19;457(7232):1012-1014. [doi: ]
Buehler JW, Berkelman RL, Hartley DM, Peters CJ. Syndromic surveillance and bioterrorism-related epidemics. EmergInfect Dis 2003 Oct;9(10):1197-1204 ]
Elliot AJ, Singh N, Loveridge P, Harcourt S, Smith S, Pnaiser R, et al. Syndromic surveillance to assess the potential publichealth impact of the Icelandic volcanic ash plume across the United Kingdom, April 2010. Euro Surveill 2010;15(23)[] ]
Ujike M, Shimabukuro K, Mochizuki K, Obuchi M, Kageyama T, Shirakura M, Working Group for Influenza VirusSurveillance in Japan. Oseltamivir-resistant influenza viruses A (H1N1) during 2007-2009 influenza seasons, Japan. EmergInfect Dis 2010 Jun;16(6):926-935 [doi: ]
National Institute for Health and Clinical Excellence. 2009 Feb. Amantadine, Oseltamivir and Zanamivir for the Treatmentof influenza: Review of NICE Technology Appraisal Guidance 58 (NICE Technology Appraisal Guidance 168) URL:[accessed 2011-06-30]
Centers for Disease Control and Prevention. 2011 Jan 31. Interim Guidance on the Use of Influenza Antiviral Agents Duringthe 2010-2011 Influenza Season [accessed 2011-06-30][]
Harper SA, Bradley JS, Englund JA, File TM, Gravenstein S, Hayden FG, Expert Panel of the Infectious Diseases Societyof America. Seasonal influenza in adults and children--diagnosis, treatment, chemoprophylaxis, and institutional outbreakmanagement: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis 2009 Apr15;48(8):1003-1032 [doi: ]
Sugawara T, Ohkusa Y, Kawanohara H, Taniguchi K, Okabe N. [The real-time pharmacy surveillance and its estimationof patients in 2009 influenza A (H1N1)]. Kansenshogaku Zasshi 2011 Jan;85(1):8-15. [Medline:
Ministry of Health, Labour and Welfare, Japan. 2010. Constructing an Appropriate, Stable and Efficient Healthcare InsuranceSystem [in Japanese] [accessed 2011-06-30][]
Sugawara T, Ohkusa Y, Kondo M, Honda Y, Okubo I. [Research on choices of people with mild symptoms of commoncold between consulting physicians and taking OTC (over-the-counter) medicine using a hypothetical question method]. Nihon Koshu Eisei Zasshi 2005 Jul;52(7):618-626. [Medline:
Wu TS, Shih FY, Yen MY, Wu JS, Lu SW, Chang KC, et al. Establishing a nationwide emergency department-basedsyndromic surveillance system for better public health responses in Taiwan. BMC Public Health 2008;8:18 ] [doi: ] [Medline:
Lazarus R, Kleinman K, Dashevsky I, Adams C, Kludt P, DeMaria A, et al. Use of automated ambulatory-care encounterrecords for detection of acute illness clusters, including potential bioterrorism events. Emerg Infect Dis 2002 Aug;8(8):753-760[] ]
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.7
(page number not for citation purposes)
Henning KJ. What is syndromic surveillance? MMWR Morb Mortal Wkly Rep 2004 Sep 24;53 Suppl:5-11 [] [Medline:
Ohkusa Y, Sugiura H, Sugawara T, Taniguchi K, Okabe N. [Symptoms of outpatients as data for syndromic surveillance]. Kansenshogaku Zasshi 2006 Jul;80(4):366-376. [Medline:
South BR, South BR, Chapman WW, Chapman W, Delisle S, Shen S, et al. Optimizing A syndromic surveillance textclassifier for influenza-like illness: Does document source matter? AMIA Annu Symp Proc 2008:692-696. [Medline:
Gundlapalli AV, Olson J, Smith SP, Baza M, Hausam RR, Eutropius LJ, et al. Hospital electronic medical record-basedpublic health surveillance system deployed during the 2002 Winter Olympic Games. Am J Infect Control 2007Apr;35(3):163-171. [doi: ]
Lewis MD, Pavlin JA, Mansfield JL, O'Brien S, Boomsma LG, Elbert Y, et al. Disease outbreak detection system usingsyndromic data in the greater Washington DC area. Am J Prev Med 2002 Oct;23(3):180-186. ]
Ministry of Health, Labour and Welfare, Japan. 2011 Jun 27. Survey of Medical Institutions [accessed 2011-06-30]
Ohkusa Y, Yamaguchi R, Sugiura H, Sugawara T, Yoshida M, Shimada C, et al. [2008 G8 Hokkaido Toyako SummitMeeting Syndrome Surveillance]. Kansenshogaku Zasshi 2009 May;83(3):236-244. ]
Mandl KD, Overhage JM, Wagner MM, Lober WB, Sebastiani P, Mostashari F, et al. Implementing syndromic surveillance:a practical guide informed by the early experience. J Am Med Inform Assoc 2004 Apr;11(2):141-150 [][doi: ] [Medline:
Lazarus R, Kleinman K, Dashevsky I, DeMaria A, Platt R. Using automated medical records for rapid identification ofillness syndromes (syndromic surveillance): the example of lower respiratory infection. BMC Public Health 2001;1:9[] ]
Kawai N, Kawade Y, Kobayashi H, Okada S, Higuchi Y, Kawaji H, et al. Analysis of influenza activity during 2009influenza pandemic A (H1N1) using real-time infectious disease surveillance in Gifu prefecture [in Japanese]. SyukanNihon Iji Shinpou 2010;4487:58-64.
Valdivia A, Lopez-Alcalde J, Vicente M, Pichiule M, Ruiz M, Ordobas M. Monitoring influenza activity in Europe withGoogle Flu Trends: comparison with the findings of sentinel physician networks - results for 2009-10. Euro Surveill2010;15(29) [] [Medline:
Ohkusa Y, Shigematsu M, Taniguchi K, Okabe N. Experimental surveillance using data on sales of over-the-countermedications--Japan, November 2003-April 2004. MMWR Morb Mortal Wkly Rep 2005 Aug 26;54 Suppl:47-52 [[Medline:
Chugai Pharmaceutical Co. Ltd. 2011 Jun 30. Tamiflu 75 [in Japanese] [accessed 2011-06-30] [
Ministry of Health, Labour and Welfare, Japan. 2008. Survey of Medical Care Activities in Public Health Insurance [inJapanese] URL: [accessed 2011-06-30] []
Abbreviations EMR: electronic medical record EPRS: electronic prescription record system Edited by G Eysenbach; submitted 30.06.11; peer-reviewed by D Zeng; comments to author 26.09.11; revised version received25.10.11; accepted 01.11.11; published 16.01.12Please cite as:Sugawara T, Ohkusa Y, Ibuka Y, Kawanohara H, Taniguchi K, Okabe NReal-time Prescription Surveillance and its Application to Monitoring Seasonal Influenza Activity in JapanJ Med Internet Res 2012;14(1):e14PMID:
Tamie Sugawara, Yasushi Ohkusa, Yoko Ibuka, Hirokazu Kawanohara, Kiyosu Taniguchi, Nobuhiko Okabe. Originallypublished in the Journal of Medical Internet Research (http://www.jmir.org), 16.01.2012. This is an open-access article distributedunder the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0/), which permitsunrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.8
(page number not for citation purposes)
Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication onhttp://www.jmir.org/, as well as this copyright and license information must be included.
J Med Internet Res 2012 | vol. 14 | iss. 1 | e14 | p.9
(page number not for citation purposes)
Lezing homeopathie voor huisartsen en apotheek-medewerkers te Oss Graag wil ik u wat vertellen over homeopathie, als een volwaardige complementaire geneeswijze, naast de reguliere. Ik mag dat na bijna 25 jaar praktijkervaring zo stellen. 1.Eerst wil ik het kort hebben over de historie, en de filosofie van de homeopathie. 2.Dan over de praktijk van alle dag, waaronder het homeopathisch cons
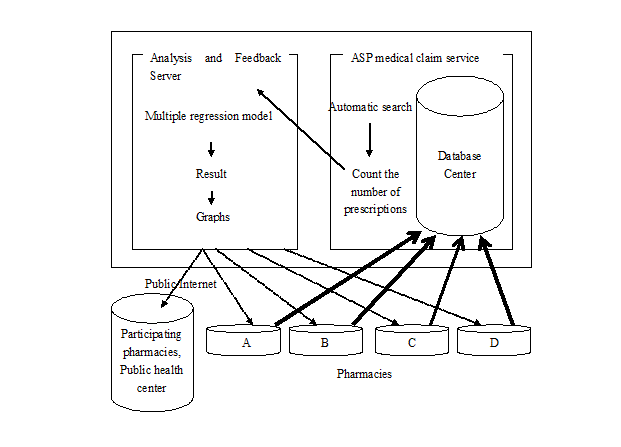 Figure 1. Prescription surveillance. Pharmacies A-D use the application service provider's (ASP) medical claims service. All data are stored in a
Figure 1. Prescription surveillance. Pharmacies A-D use the application service provider's (ASP) medical claims service. All data are stored in a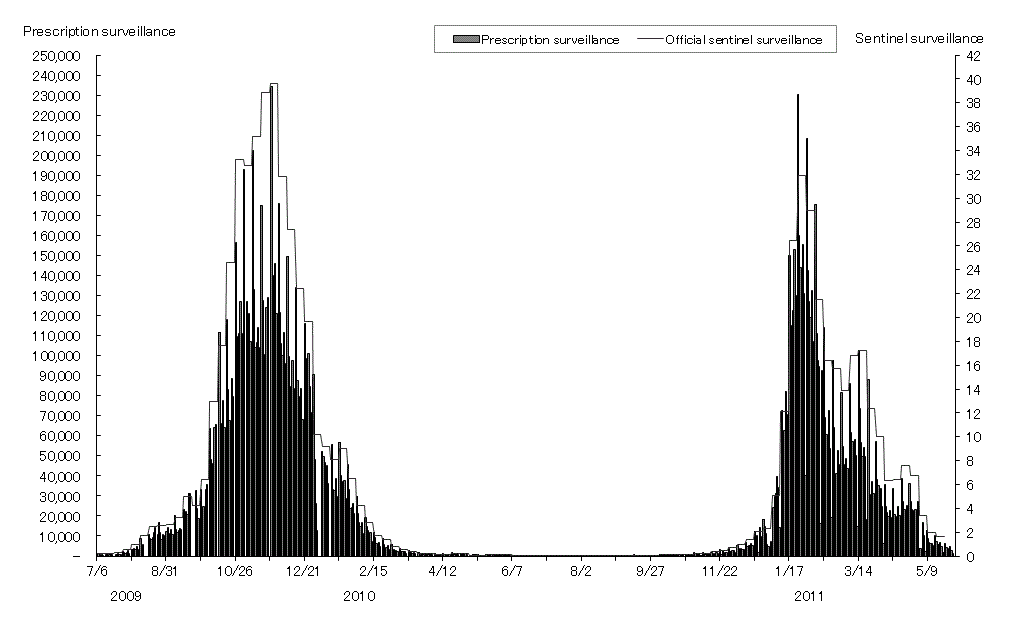 surveillance estimated the total number of patients for the same
(95% confidence interval 13,350,000-14,010,000) for the
2010-2011 influenza seasons [indicating that the sentinel
20,460,000-20,860,000) for the 2009-2010 and 13,680,000
estimates were approximately double our estimates.
surveillance estimated the total number of patients for the same
(95% confidence interval 13,350,000-14,010,000) for the
2010-2011 influenza seasons [indicating that the sentinel
20,460,000-20,860,000) for the 2009-2010 and 13,680,000
estimates were approximately double our estimates.