L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Sharc.sums.ac.ir
Metab Brain Dis (2008) 23:485-492DOI 10.1007/s11011-008-9109-2
Effects of the HIV treatment drugs nevirapineand efavirenz on brain creatine kinase activity
Emilio L. Streck & Giselli Scaini & Gislaine T. Rezin &Jeverson Moreira & Celine M. Fochesato &Pedro R. T. Romão
Received: 2 June 2008 / Accepted: 15 August 2008 /Published online: 24 September 2008
# Springer Science + Business Media, LLC 2008
Abstract Nevirapine (NVP) and efavirenz (EFV) are antiretroviral drugsbelonging to potent class of non-nucleoside reverse transcriptase inhibitors(NNRTIs) widely used for the treatment human immunodeficiency virus (HIV)infection. It has been demonstrated that NVP and EFV are able to cross theblood-brain barrier and arrive at the central nervous system (CNS), causingimportant adverse effects related to their presence within this tissue. Consid-ering that the exact mechanisms responsible for CNS toxicity associated withNVP and EFV remain unknown and that creatine kinase (CK) plays animportant role in cell energy homeostasis, in the present work we evaluated CKactivity in brain of mice after chronic administration of these drugs. Our resultsdemonstrated that NVP and EFV significantly inhibited CK activity incerebellum, hippocampus, striatum and cortex of mice. Although it is difficultto extrapolate our findings to the human condition, the inhibition of brain CKactivity by NVP and EFV may be associated with neurological adversesymptoms of these drugs.
Keywords Antiretroviral drugs. Efavirenz. Nevirapine. Creatine kinase
E. L. Streck G. Scaini G. T. RezinLaboratório de Fisiopatologia Experimental, Unidade Acadêmica de Ciências da Saúde,Programa de Pós-graduação em Ciências da Saúde, Universidade do Extremo Sul Catarinense,Criciúma, SC, Brazil
J. Moreira C. M. Fochesato P. R. T. Romão (*)Laboratório de Imunologia e Mutagênese, Unidade Acadêmica de Ciências da Saúde,Programa de Pós-graduação em Ciências da Saúde, Universidade do Extremo Sul Catarinense,Criciúma, SC, Brazile-mail: ptr@unesc.net
Nevirapine (NVP) and efavirenz (EFV) are antiretroviral drugs belonging to potentclass of non-nucleoside reverse transcriptase inhibitors (NNRTIs), drugs currentlyused as part of highly active antiretroviral therapy (HAART) regimen. They arerecommended at initial therapy for asymptomatic HIV patients or in advanceddisease and also in patients presenting with failure of antiretroviral therapy (Dybul etal. The HAART completely changed the clinical evolution of HIV infection,reducing the morbidity and mortality among HIV-1 infected patients and changingthe incidence of neurological complications in acquired immunodeficiency syn-drome (AIDS) patients (Dore et al. ; Sacktor et al. ). Nevertheless, drugrelated toxicity is one of the obstacles in the fight against AIDS (von Giesen et al. ).
It was well demonstrated that both NNRTIs, NVP and EFV, are able to cross the
blood-brain barrier and enter the central nervous system (CNS) (von Giesen et al. ; Treisman and Kaplin and possibly cause important adverse effectsrelated to their presence within this tissue, especially EFV (Bickel et al. ;Arendt et al. ; Maggiolo ).
NVP is the oldest NNRTI offering a better treatment compliance due to its once
daily initial dosage (only for the first 2 weeks, after that the dosage goes to twicedaily). Despite this advantage, side effects such as hypersensitivity reaction, gastriccomplications and hepatotoxicity can be frequently observed. Futhermore, neuro-psychiatry complications have been associated with its use (Wise et al. ).
EFV is known by its efficacy and easy treatment compliance. However, it was
observed that more than 50% of patients receiving EFV reported neurologicaladverse symptoms which are very specific of this NNRTI. CNS side effectsincluding insomnia, dizziness, impaired concentration, vertigo, depression, abnormaldreams and hallucinations are very frequent during the first week of therapy(Treisman and Kaplin ; Bickel et al. Adkins and Noble ; Gutiérrez etal. ). Recent studies have demonstrated that neuropsychiatry disorders maypersist in patients chronically treated with EFV (Fumaz et al. ; Rihs et al. The exact mechanism responsible for CNS toxicity associated with EFV remainsunknown, but plasma and intracellular drug concentrations and CYP2B6 genotypehave been found to be predictors of early neuropsychological disturbances inpatients starting antiretroviral therapy regimens containing EFV (Haas et al. ;Gutiérrez et al.
Although HAART regimen represents a very important role in the treatment of
HIV/AIDS, its side effects can be responsible for patients' non adherence to drugs,contributing to the treatment failure and development of resistant HIV strains(Piacenti
Creatine kinase (CK; E.C. 2.7.3.2) catalyzes the reversible transfer of a
phosphoryl group from ATP to creatine, producing phosphocreatine and ADP(Bessman and Carpenter Wallimann et al. ). This enzyme plays animportant role in the rapid regeneration of ATP in high-energy consuming tissuessuch as brain, skeletal muscle and heart, where it functions as an effective bufferingsystem of cellular ATP levels. In this context, it has been widely shown that adecrease in CK activity is associated with a neurodegenerative pathway that results
in neuronal loss following brain ischemia (Tomimoto et al. neurodegenerativediseases (David et al. ; Aksenov et al. and other pathological states(Gross et al. ; Streck et al. ). Moreover, we have recently demonstrated thatbrain CK activity is altered by antipsychotic (Assis et al. electroconvulsiveschock (Búrigo et al. and ruthenium compounds (Zanette et al. ).
Therefore, considering that CK plays an important role in cell energy
homeostasis, that impairment of brain metabolism is linked to neuronal death andthat NVP and mainly EFV-treated patients present important CNS adverse effects, inthe present work we evaluated CK activity in brain of mice after chronicadministration of these drugs.
Animals Male CF-1 mice (age 60-90 days; weight 30-40 g) were obtained from theState Foundation for Health Science Research (FEPPS-RS, Porto Alegre, Brazil),and maintained in the animal facility of Universidade do Extremo Sul Catarinense(UNESC) for at least 2 weeks before drug treatment. The animals were housed inplastic cages, eight per cage, under 12 h light/dark cycle (lights on 7:00 A.M.) atconstant room temperature of 23±1°C; with water and food ad libitum. Allexperimental procedures were carried out in accordance with the National Institutesof Health Guide for the Care and Use of Laboratory Animals and the BrazilianSociety for Neuroscience and Behavior (SBNeC) recommendations for animal care,with the approval of local Ethics Committee.
Drugs and treatment Two NNRTIs were employed in this study: efavirenz (EFV-Patheon Inc., Mississauga, Ontario, Canada) and nevirapine (NVP-BoehringerIngelheim Roxane, Inc. Columbus, Ohio, USA). Normal mice were treated orally,once a day for 36 days, with EFV 10 mg/kg, NVP 3.3 mg/kg or vehicle in a volumeof 1 mL/kg. The doses employed in this study were based on the doses used forhuman therapy (Lewis et al. ). EFV and NVP were dissolved in distillated waterslightly warmed with Tween 80 1%. The control group received a solution consistingof distillated water with Tween 80 1%. Drug solutions were prepared daily justbefore the oral administration. The animals were killed by decapitation 3 h after thelast administration of the drugs. The brain was immediately removed andhippocampus, striatum, cerebellum, cortex and prefrontal cortex were isolated.
Tissue and homogenate preparation These brain areas were homogenized (1:10,w/v) in SETH buffer, pH 7.4 (250 mM sucrose, 2 mM EDTA, 10 mM Trizmabase, 50 IU/ml heparin). The homogenates were centrifuged at 800×g for 10 minand the supernatants kept at −70°C until used for CK activity determination. Themaximal period between homogenate preparation and enzyme analysis wasalways less than 5 days. Protein content was determined by the method describedby Lowry et al. (using bovine serum albumin as standard.
Creatine kinase (CK) activity assay Creatine kinase activity was measured in brainhomogenates pre-treated with 0.625 mM lauryl maltoside. The reaction mixture
consisted of 60 mM Tris-HCl, pH 7.5, containing 7 mM phosphocreatine, 9 mMMgSO4 and approximately 0.4-1.2 μg protein in a final volume of 100 μL. After15 min of pre-incubation at 37°C, the reaction was started by the addition of0.3 μmol of ADP plus 0.08 μmol of reduced glutathione. The reaction was stoppedafter 10 min by the addition of 1 μmol of p-hydroxymercuribenzoic acid. Thecreatine formed was estimated according to the colorimetric method of Hughes). The color was developed by the addition of 100 μL 2% α-naphtol and100 μL 0.05% diacetyl in a final volume of 1 mL and read spectrophotometricallyafter 20 min at 540 nm. Results were expressed as nmol/min.mg protein.
Statistical analysis Data were analyzed by one-way analysis of variance (ANOVA)followed by the Tukey test when F was significant and are expressed as mean ±standard deviation. All analyses were performed using the Statistical Package for theSocial Science (SPSS) software.
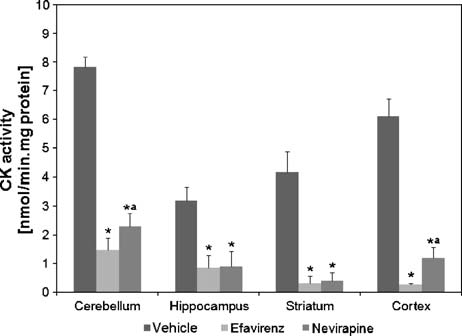
In this study we treated mice for 36 days with antiretroviral drugs at doses similar tothose administrated in humans. As seen in Fig. , our results demonstrated that EFVand NVP significantly inhibited creatine kinase activity in cerebellum (F(2,12)=328.9; p<0.01), hippocampus (F(2,12) =38.2; p<0.01), striatum (F(2,12) =103.7; p<0.01) and cortex (F(2,12) =296.9; p<0.01) of mice. Futhermore, we observed thatanimals treated with EFV presented more intense inhibition on CK in cortex andcerebellum when compared to the group treated with NVP. We also observed thatNVP-treated group showed a reduction of approximately 17% in body weight at theend of treatment, when compared to the beginning (data not shown).
Fig. 1 Creatine kinase (CK) activity in the cerebellum, hippocampus, striatum and cerebral cortex of micesubmitted to chronic administration of efavirenz and nevirapine. Data are expressed as units per milligramprotein, for five independent experiments (n=5) performed in duplicate. Different from control (vehicle)*p<0.01 (Tukey test). Different from EFV-treated group ap<0.05 (Tukey test)
Although non-nucleoside analogue inhibitors of HIV-1 reverse transcriptase (RT)have become a cornerstone of antiretroviral combination regimens during HAART,adverse events CNS-related can be responsible for patients' non-adherence tomedications (Piacenti ).
There are some reports suggesting that neuropsychiatric features like anxiety,
hostility and depression seen in patients with long-term EFV use were associatedwith high serum drug concentration (Gutiérrez et al. Rihs et al. ;Marzolini et al. ; Hawkins et al. ). On the other hand, indirect evidencesuggests that NVP reaches the CNS comes from the headaches and neuropsychiatriccomplications sometimes associated with its use (Wise et al.
Drugs must cross the blood-brain and blood-cerebrospinal fluid (CSF) barriers to
reach the CNS. In this context, there are direct clinical evidences that the NNRTIsare able to penetrate the CSF, and for NVP, the CSF/plasma ratio has been reportedto range from 15 to 40% (von Giesen et al. ; van Praag et al. ). Gibbs et al. ) have demonstrated that NVP accumulates in the brain, CSF, choroid plexusand brain parenchyma of guinea pig. In addition, both EFV and NVP can be detectedin the cerebrospinal fluid in concentrations effective in suppressing HIV viral levels(Tashima et al. ; Wynn et al. ), which might be a prerequesite for theproven CNS efficacy or for the manifestations of CNS side effects. The degree ofNVP brain uptake was higher for an antiviral HIV drug. In fact, NVP has the highestbrain accumulation of any of the antiretroviral drugs tested, including abacavir,amprenavir and ritonavir (Anthonypillai et al. ; Anthonypillai et al. ).
In the present paper, we demonstrated that EFV and NVP significantly inhibited
CK activity in cerebellum, hippocampus, striatum and cortex of mice. Moreover, CKactivity in cortex and in cerebellum was significantly lower in EFV-treated groupwhen compared to NVP-treated group. This could explain a diference in neurologictolerability of the two drugs. In order to ellucidate this hypothesis further studiesneed to be done. We did not investigate the plasmatic or cerebrospinal fluidconcentrations of NNRTIs, but as commented above, both drugs have a good CNSpenetration (Tashima et al. Wynn et al. ; Gibbs et al. ).
CK is important for normal energy homeostasis by exerting several integrated
functions, such as temporary energy buffering, metabolic capacity, energy transferand metabolic control (Wallimann et al. The brain, like other tissues withhigh and variable rates of ATP metabolism, presents high phosphocreatineconcentration and CK activity. It is well described that inhibition of CK activityhas been implicated in the pathogenesis of a number of diseases, especially in brain(Khuchua et al. ; Schlattner and Wallimann Energy impairment has beenlinked to neuronal death and neurodegeneration (Heales et al. ; Blass ;Schurr ). In this context, it has also been demonstrated that the creatine/phosphocreatine/CK circuit is involved in processes that involve habituation,spatial learning and seizure susceptibility (Jost et al. Streijger et al. ;Streijger et al.
The mechanisms underlying NNRTIs side effects are still poorly understood. In
the present work, we demonstrated, for the first time, that brain CK activity wasinhibited in cerebellum, hippocampus, striatum and cortex when mice were
chronically treated with any of the NNRTIs, EFV or NVP. The clinical correlationwith activity and behavior of mice should be further more investigated.
This work was supported by grants from Conselho Nacional de Desenvolvimento
Científico e Tecnológico (CNPq), Fundação de Apoio à Pesquisa Científica e Tecnológica do Estado deSanta Catarina (FAPESC) and Universidade do Extremo Sul Catarinense (UNESC).
Adkins JC, Noble S (1998) Efavirenz. Drugs 56:1055-1064Aksenov M, Butterfield DA, Markesbery WR (2000) Oxidative modification of creatine kinase BB in
Alzheimer's disease brain. J Neurochem 74:2520-2527
Anthonypillai C, Sanderson RN, Gibbs JE, Thomas SA (2004) The distribution of the HIV protease
inhibitor, ritonavir, to the brain, cerebrospinal fluid, and choroid plexuses of the guinea pig. JPharmacol Exp Ther 308:912-920
Anthonypillai C, Gibbs JE, Thomas SA (2006) The distribution of the anti-HIV drug, tenofovir
(PMPA), into the brain, CSF and choroid plexuses. Cerebrospinal Fluid Res 3:1-10
Arendt G, de Nocker D, von Giesen HJ, Nolting T (2007) Neuropsychiatric side effects of efavirenz
therapy. Expert Opin Drug Saf 6:147-154
Assis LC, Scaini G, Di-Pietro PB, Castro AA, Comim CM, Streck EL, Quevedo J (2007) Effect of
antipsychotics on creatine kinase activity in rat brain. Basic Clin Pharmacol Toxicol 101:315-319
Bessman SP, Carpenter CL (1985) The creatine-creatine phosphate energy shuttle. Annu Rev Biochem
Bickel M, Stephan C, Rottmann C, Carlebach A, Haberl A, Kurowski M, Staszewski S (2005) Severe
CNS side-effect and persistent high efavirenz plasma levels in a patient with HIV/HCV coinfectionand liver cirrhosis. Scand J Infect Dis 37:520-522
Blass JP (2001) Brain metabolism and brain disease: is metabolic deficiency the proximate cause of
Alzheimer dementia? J Neurosci Res 66:851-856
Búrigo M, Roza CA, Bassani C, Feier G, Dal-Pizzol F, Quevedo J, Streck EL (2006) Decreased
creatine kinase activity caused by electroconvulsive shock. Neurochem Res 31:877-881
David S, Shoemaker M, Haley BE (1998) Abnormal properties of creatine kinase in Alzheimer's
disease brain: correlation of reduced enzyme activity and active site photolabeling with aberrantcytosol-membrane partitioning. Mol Brain Res 54:276-287
Dore GJ, Correll PK, Li Y, Kaldor JM, Cooper DA, Brew BJ (1999) Changes to AIDS dementia
complex in the era of highly active antiretroviral therapy. AIDS 13:1249-1253
Dybul M, Fauci AS, Bartlett JG, Kaplan JE, Pau AK (2002) Panel on clinical practices for the
treatment of HIV. Guidelines for using antiretroviral agents among HIV-infected adults andadolescents. Recommendations of the panel on clinical practices for treatment of HIV. MMWRRecomm Rep 51:1-55
Fumaz CR, Munõz-Moreno JA, Moltó J, Negredo E, Ferrer MJ, Sirera G, Pérez-Alvarez N, Gómez
G, Burger D, Clotet B (2005) Long-term neuropsychiatric disorders on efavirenz-basedapproaches: quality of life, psychologic issues, and adherence. J Acquir Immune Defic Syndr38:560-565
Gibbs JE, Gaffen Z, Thomas SA (2006) Nevirapine uptake into the central nervous system of the Guinea
pig: an in situ brain perfusion study. J Pharmacol Exp Ther 317:746-751
Gross WL, Bak MI, Ingwall JS, Arstall MA, Smith TW, Balligand JL, Kelly RA (1996) Nitric oxide
inhibits creatine kinase and regulates rat heart contractile reserve. Proc Natl Acad Sci USA 93:5604-5609
Gutiérrez F, Navarro A, Padilla S, Antón R, Masiá M, Borrás J, Martín-Hidalgo A (2005) Prediction
of neuropsychiatric adverse events associated with long-term efavirenz therapy, using plasma druglevel monitoring. Clin Infect Dis 41:1648-1653
Haas DW, Ribaudo HJ, Kim RB, Tierney C, Wilkinson GR, Gulick RM Clifford DB, Hulgan T,
Marzolini C, Acosta EP (2004) Pharmacogenetics of efavirenz and central nervous system sideeffects: an adult AIDS clinical trials group study. AIDS 18(18):2391-2400
Hawkins T, Geist C, Young B, Giblin A, Mercier RC, Thornton K, Haubrich R (2005) Comparison of
neuropsychiatric side effects in an observational cohort of efavirenz- and protease inhibitor-treatedpatients. HIV Clin Trials 6:187-196
Heales SJ, Bolaños JP, Stewart VC, Brookes PS, Land JM, Clark JB (1999) Nitric oxide, mitochondria
and neurological disease. Biochim Biophys Acta 1410:215-228
Hughes BP (1962) A method for estimation of serum creatine kinase and its use in comparing creatine
kinase and aldolase activity in normal and pathologic sera. Clin Chim Acta 7:597-604
Jost CR, Van der Zee CE, Zandt HJ, Oerlemans F, Verheij M, Streijger F, Fransen J, Heerschap A, Cools
AR, Wieringa B (2002) Creatine kinase B-driven energy transfer in the brain is important forhabituation and spatial learning behaviour, mossy fibre field size and determination of seizuresusceptibility. Eur J Neurosci 15:1692-1706
Khuchua ZA, Qin W, Boero J, Cheng J, Payne RM, Saks VA, Strauss AW (1998) Octamer formation and
coupling of cardiac sarcomeric mitochondrial creatine kinase are mediated by charged N-terminalresidues. J Biol Chem 273:22990-22996
Lewis W, Kohler JJ, Hosseini SH, Haase CP, Copeland WC, Bienstock RJ Ludaway T, McNaught J, Russ
R, Stuart T, Santoianni R (2006) Antiretroviral nucleosides, deoxynucleotide carrier and mitochon-drial DNA: evidence supporting the DNA pol gamma hypothesis. AIDS 20:675-684
Lowry OH, Rosebrough NJ, Farr AL, Randall RJ (1951) Protein measurement with the Folin phenol
Maggiolo F (2007) Efavirenz. Expert Opin Pharmacoter 8(8):1137-1145Marzolini C, Telenti A, Decosterd LA, Greub G, Biollaz J, Buclin T (2001) Efavirenz plasma levels can
predict treatment failure and central nervous system side effects in HIV-1-infected patients. AIDS15:71-75
Piacenti FJ (2006) An update and review of antiretroviral therapy. Pharmacotherapy 26:1111-1133Rihs TA, Begley K, Smith DE, Sarangapany J, Callaghan A, Kelly M, Post JJ, Gold J (2006) Efavirenz
and chronic neuropsychiatric symptoms: a cross-sectional case control study. HIV Med 7:544-548
Sacktor N, Lyles RH, Skolasky R, Kleeberger C, Selnes OA, Miller EN, Becker JT, Cohen B, McArthur
JC (2001) HIV-associated neurologic disease incidence changes: multicenter AIDS cohort study,1990-1998. Neurology 56:257-260
Schlattner U, Wallimann T (2000) Octamers of mitochondrial creatine kinase isoenzymes differ in stability
and membrane binding. J Biol Chem 275:17314-17320
Schurr A (2002) Energy metabolism, stress hormones and neural recovery from cerebral ischemia/
Streck EL, Amboni G, Scaini G, Di-Pietro PB, Rezin GT, Valvassori SS, Luz G, Kapczinski F,
Quevedo J (2008) Brain creatine kinase activity in an animal model of mania. Life Sci 82:424-429
Streijger F, Jost CR, Oerlemans F, Ellenbroek BA, Cools AR, Wieringa B, Van der Zee CE (2004)
Mice lacking the UbCKmit isoform of creatine kinase reveal slower spatial learning acquisition,diminished exploration and habituation, and reduced acoustic startle reflex responses. Mol CellBiochem 256/257:305-318
Streijger F, Oerlemans F, Ellenbroek BA, Jost CR, Wieringa B, Van der Zee CE (2005) Structural and
behavioural consequences of double deficiency for creatine kinases BCK and UbCKmit. Behav BrainRes 157:219-234
Tashima KT, Caliendo AM, Ahmad M, Gormley JM, Fiske WD, Brennan JM, Flanigan TP (1999)
Cerebrospinal fluid human immunodeficiency virus type 1 (HIV-1) suppression and efavirenzdrug concentrations in HIV-1-infected patients receiving combination therapy. J Infect Dis180:862-864
Tomimoto H, Yamamoto K, Homburger HA, Yanagihara T (1993) Immunoelectron microscopic
investigation of creatine kinase BB-isoenzyme after cerebral ischemia in gerbils. Acta Neuropathol86:447-455
Treisman GJ, Kaplin AI (2002) Neurologic and psychiatric complications of antiretroviral agents. AIDS
van Praag RM, van Weert EC, van Heeswijk RP, Zhou XJ, Sommadossi JP, Jurriaans S, Lange JM,
Hoetelmans RM, Prins JM (2002) Stable concentrations of zidovudine, stavudine, lamivudine,abacavir, and nevirapine in serum and cerebrospinal fluid during 2 years of therapy. AntimicrobAgents Chemother 46:896-899
von Giesen HJ, Köller H, Theisen A, Arendt G (2002) Therapeutic effects of nonnucleoside reverse
transcriptase inhibitors on the central nervous system in HIV-1-infected patients. J Acquir ImmuneDefic Syndr 29:363-367
Wallimann T, Wyss M, Brdiczka D, Nicolay K, Eppenberger HM (1992) Intracellular compartmen-
tation, structure and function of creatine kinase isoenzymes in tissues with high and fluctuatingenergy demands: the 'phosphocreatine circuit' for cellular energy homeostasis. Biochem J 281:21-40
Wise ME, Mistry K, Reid S (2002) Drug points: neuropsychiatric complications of nevirapine treatment.
Wynn HE, Brundage RC, Fletcher CV (2002) Clinical implications of CNS penetration of antiretroviral
Zanette F, Victor EG, Scaini G, Di-Pietro PB, Cardoso DC, Cristiano MP, Dal-Pizzol F, Paula MM, Streck
EL (2007) Modulation of creatine kinase activity by ruthenium complexes. J Inorg Biochem 101:267-273
Pharmavantage MATERIAL SAFETY DATA SHEET FEXOFENADINE HYDROCHLORIDE Date Updated: 02/08/2005 Section 1 - Product and Company Information Product Name FEXOFENADINE HYDROCHLORIDE Manufacturer: Excel Pharmaceutical Co., Ltd Emergency Phone: +86-10-85271798 Fax: +86-10-85271100 Section 2 - Composition/Information on Ingredient Substance Name FEXOFENADINE HYDROCHLORIDE CAS #83799-24-0 Formula C32H39NO4
Disfunzione del SNV, Diabete Mellito tipo 2 e Cardiopatia Ischemica nella Sindrome Metabolica. Effetti della Melatonina. Introduzione. Nella prevenzione primaria delle componenti della Sindrome Metabolica, realizzata clinicamente con la Semeiotica Biofisica Quantistica utilizzando come suo fondamento la dieta, intesa in senso etimologico, la melatonina e altri preparati istangioprotet
 consisted of 60 mM Tris-HCl, pH 7.5, containing 7 mM phosphocreatine, 9 mMMgSO4 and approximately 0.4-1.2 μg protein in a final volume of 100 μL. After15 min of pre-incubation at 37°C, the reaction was started by the addition of0.3 μmol of ADP plus 0.08 μmol of reduced glutathione. The reaction was stoppedafter 10 min by the addition of 1 μmol of p-hydroxymercuribenzoic acid. Thecreatine formed was estimated according to the colorimetric method of Hughes). The color was developed by the addition of 100 μL 2% α-naphtol and100 μL 0.05% diacetyl in a final volume of 1 mL and read spectrophotometricallyafter 20 min at 540 nm. Results were expressed as nmol/min.mg protein.
consisted of 60 mM Tris-HCl, pH 7.5, containing 7 mM phosphocreatine, 9 mMMgSO4 and approximately 0.4-1.2 μg protein in a final volume of 100 μL. After15 min of pre-incubation at 37°C, the reaction was started by the addition of0.3 μmol of ADP plus 0.08 μmol of reduced glutathione. The reaction was stoppedafter 10 min by the addition of 1 μmol of p-hydroxymercuribenzoic acid. Thecreatine formed was estimated according to the colorimetric method of Hughes). The color was developed by the addition of 100 μL 2% α-naphtol and100 μL 0.05% diacetyl in a final volume of 1 mL and read spectrophotometricallyafter 20 min at 540 nm. Results were expressed as nmol/min.mg protein.