L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Petzold-errors-communication
Errors, communication and a learning feedback-loop for development Structure:
2) 'Personal medicine' considers the feedback-loop of communicative self-
Different criteria for errors
Before we talk about how to handle or avoid 'medical errors' we should clarify what
Is it an error, when a doctor doesn't diagnose an angina caused by streptococcus A,
when a child has a sore throat, and does not prescribe penicillin? Is it still an error,
when the child becomes healthy after a week? Was it an error, when the child gets
an endocarditis rheumatica after two weeks? Or on the other way: when the doctor
diagnoses a streptococcus infection and prescribe penicillin and the child gets an
allergic shock - was at a medical error? Or the streptococcus become resistant
against penicillin and the child gets an endocarditis - was it an error?
Criteria for defining errors are related to the desired outcome of the medical
interventions. Analogous to the doctor's aims the criteria for errors differ at least in
three categories: 1. Well-being of the patient, 2. Disappearance of the symptoms or
disease, and 3. Diagnosis and treatment corresponding to a cultural defined standard
In relation to the attractive goal you take in the centre of your attention and your
intention you will find different kinds of errors with different kinds of harm. In our
example with the child with sore throat there is no error under 1st and 2nd criterion,
when the child becomes and stays healthy again after one week - unconsidered it
got penicillin or not. There is an error, when the child gets a complication of this
infection also under the 1st and 2nd criterion. Under the 3rd criterion there is an error
when it doesn't get antibiotics, unconsidered it gets healthy or a complication. And
when the doctor prescribes penicillin, it was an error under the 1st criterion, but not
under the 2nd and 3rd, when the child gets allergic or severe intestinal reactions.
So you can see, a doctor is acting always in the dilemma, that - so it seems to make
no difference what he is doing - he only can make mistakes, either in the eye of the
patient or under the criterion of EBM; and this even in such a simple daily case of
The angina itself doesn't need a specific treatment but only the danger of
complications requires antibiotics. It becomes not only a complicated but also a
Petzold, Theodor: Errors, Communication… 30.06.2013 -1-
complex problem, when we try to consider the individual constitution for possible
complications of our treatment decision. Later we will see how shared decision
making helps us in those cases to make less errors or at least errors with less severe
But first we will take it as simple as many people (even health-professionals) see it:
There are streptococcus A as the cause of sore throat and scarlet fever with
sometimes rheumatic endocarditis etc. We can fight these bacteria with penicillin
and evaluate the outcome. The positive effect is about 70 %. Here is not the place to
discuss the outcome in detail compared with other antibiotics. I take this only as an
example to illustrate a very (may be the most) common way to think about causal
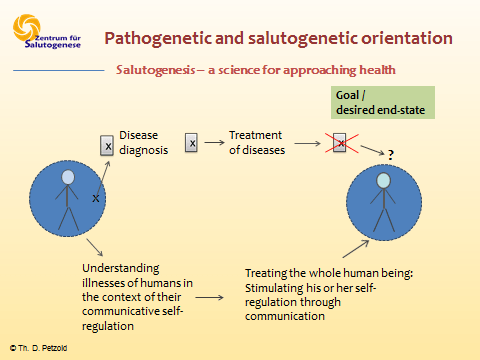
medical treatment of diseases. Summing up, it may be said, that a common way of
medical statistical logic takes this way: First you have to make the right disease
diagnosis, than you have to find the means against this disease and at last you hope
This way of medical procedure we can call a "short circuit decision making"
analogous to the electric short circuit, because it uses the very short cut from disease
diagnosis to the treatment - like a computer can do it - without observing the
patients conditions. Most of research is done in this 'short circuit treatment' and
their results we find in the EBM and in the number needed to treat NNT.
May be, that we can recognize the level of systemic errors by looking at the number
needed to treat NNT. The NNT shows us that a treatment benefit for one person
costs the harm of other persons (adverse effects, material costs). So the benefit for
one person statistically depends on the errors in the treatment of several other
persons. The NNT by hypertension with a beta-blocker or … is posed with 86 by an
outcome of a longer life, and 35 by an outcome of a stroke (…??). So - looking for a
longer life - 85 people have to take the medicine in vain therefore one is a winner.
About 13 patients of the 86 suffer about side-effects of the medicine. So the NNT
gives us an idea of systemic errors in treatment of hypertension. Under
the 1st criterion we have about 13 errors and 2-3 hits (included the fewer
strokes). Under the 2nd criterion we find nearly only hits (the symptom of
high blood pressure disappears) and the same under the 3rd.
For example it is obvious in the case of hypertension or a tumour, that disappears by
medical treatment resp. after operation and chemo-therapy, and in contrast the
patient may suffer from the side effects of the treatment more than from the
Petzold, Theodor: Errors, Communication… 30.06.2013 -2-
Do we need a new strategy for more complex cases?
This 'short circuit strategy' works quite well, if the disease is mainly determined by a
limited circumstance they figured out as a cause, like bacteria, a poison, tumour,
bullet, deficiency of a hormone, vitamin or mineral etc. This strategy doesn't work
well, if the disease in regard to health is mainly determined by more complex and
interacting individual and socio-cultural factors like distress, lifestyle, motivation and
behaviour etc., e.g. hypertension, diabetes type 2, many cases of cancer, many
mental disorders etc. In all these cases - and these are about 60-80 % of the patients
of a general practice and internal medicine and even more in the treatment of elder
people (e.g. by Medicare recipients) - it seems we need a different strategy, a new
way of thinking about treatment and have to work out a corresponding practice. This
new strategy should include and consider the personal conditions, how you can find
them in the dynamic model of communicative healthy self-regulation. It is a model of
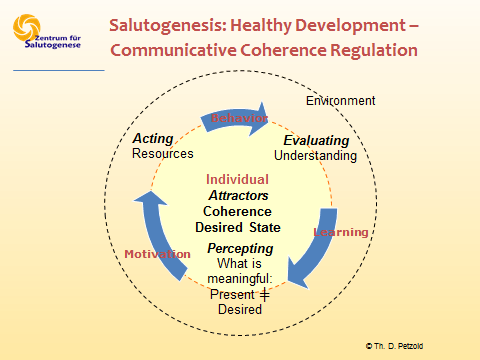
This healthy feedback-loop of self-regulation starts with perceiving the discrepancy
between the desired state ('attractor', the goal) and the present state. In a
physiological dimension, for example, one perceives the discrepancy between
present blood-sugar level (say 60 mg %) and the desired value of 100 mg%. If it is
meaningful hunger ensues and one becomes motivated to look for something to eat.
In this discrepancy between desired and present state (e.g. well-being and suffering)
we find the motivational aspect of meaningfulness. Meaningfulness can be a
physical, emotional, cultural, or spiritual issue. That depends on the at a time for a
In the feedback-loop the step following the perception of meaningfulness and the
connected motivation is that of action, the pursuit of the (aim?) goal - the advance
towards the attractor - like health. This action is regarded as "manageability".
For example, every breath we take shows the pursuit of the desired values of oxygen
and acidity in our blood. After breathing or eating our organism evaluates whether
the action was successful: Am I closer to my desired state? Or was the inhaled air bad
for my lungs? Am I still hungry following my meal or am I satisfied? Or do I feel sick?
With regard to the evaluation we learn in order to prepare for upcoming similar
situations. So if I feel sick after meal I will surely eat something different the next
time I'm hungry. In this phase we can recognize errors and learn from them.
Petzold, Theodor: Errors, Communication… 30.06.2013 -3-
So many patients have made already good and bad experiences with different
diseases and treatments. At last they have to take the medicine, or to walk, or to eat
diet… So we have to bear in mind their self-regulation, their wishes and resources.
The same feedback-loop of communicative self-regulation is active in all systems and
dimensions of life, the physical/somatic, social/emotional, the cultural/mental and
the global/universal/spiritual dimensions.
Regarding the theme of this conference: when we recognize the discrepancy
between our medical aim of healthiness and the huge number of 'adverse events' we
begin to learn - remembering our attractive aim.
So the required strategy for treating patients suffering of more complex conditions
focuses the healthy self-regulation and strives to stimulate and promote it. Diseases
and illnesses are not seen any longer as separable entities but as dynamical
interactive processes of human beings, which we desire to progress in direction of
Therapists accompany patients during their self-regulated healthy
development by communication. At first they reflect and evaluate why the patient
needs help (anamnesis). Then they perceive the actual state (self-perception and
examination by the doctor). In the next phase they look for the resources they have
for treatment, for managing the next step towards health and make a shared
decision. At last in the consultation you can already make an evaluation by imaging
the result of your action resp. treatment. At the next appointment you will do the
How we can learn from errors quickly and minimize severe sequelae of errors
In this way of communication you can find many possible errors before they happen
by imaging, and other errors like adverse effects you can find very early when you
take account of the patient's self-perception seriously. So we can use the implicit
knowledge of the patients by evaluating a planned activity in imagination.
For example: We make a shared decision that the patient will walk each day for 30
minutes and take a beta-blocker to treat his hypertension. Then we ask him or her to
imagine these actions in their daily life: are they coherent with their feeling and with
their daily routine? One may answer that he is afraid to take the beta-blocker in
cause of the side effects and another may answer that he prefer to stay in bed in the
morning than to walk. So we can change eventually the decision before acting out a
possible error (may be also an inadherence). Thus, the doctor-patient communication
Petzold, Theodor: Errors, Communication… 30.06.2013 -4-
in this way ('salutogenic communication') is a cooperative learning feedback-loop for
Another example is Mr. Leo A., a 42 years old carpenter with higher business-goals.
He was suffering of a high-tone tinnitus on his right side. The ENT-physician couldn't
find pathological variances and suggested him ten infusions and pentoxyfillin for
three months. Leo A. refused that suggestion and we talked about his ear noise in
detail. It appears when he has stressful appointments and it disappears, when he
gets a relaxing rest after lunch (reflecting). So he is motivated to change his lifestyle
in regard to a well-feeling rhythm of relaxation and a concentrate working. Ensuing
this dialogue he hasn't had a problem with tinnitus.
The error of the ENT-physician is obvious. It happens, when we act following the
'short circuit decision making' from a disease diagnosis to a treatment without
acknowledging the individual conditions.
Conclusion
If we appreciate the perceiving of our patient, and demand and promote it, and
complete it with our findings, we minimize errors in the diagnosis. By this way we
even make a new type of holistic diagnosis possible, which include the resources and
the self-healing-capacity of the patient.
When we understand medical care as salutogenically accompanying the patients in
their healthy self-regulation and as a stimulation of this development, we can use the
implicit and explicit capacity and skills of the patient as resources for the pursuit of
the health goals. The relationship between doctor and patient is a cooperative one.
The doctor asks the patient for subjective perceptions considering the development
of the healing process resp. side effects very early. In this way of salutogenic
communication the decrease of errors with undesired severe harms will be a desired
In a cultural systemic dimension we can reflect and evaluate the systemic medical
way of treatment based on the statistical EBM. We have to know the outcome of
standardised disease treatment compared with individual regarded personal
treatment under the attractive criteria of 'years of well-being'. Only by this
comparison we will be able to recognize the possible real volume of the systemic
error and will be able to learn for an advance in a more effective medicine.
E.g. the sore throat: We have to compare the outcomes of
1. every child with streptococcus-A-angina gets penicillin, with
2. personal treatment, which take account of the child's conditions, the quality of
cooperation (adherence, perception and control examinations, anxiety, stress of the
Here we need much research to find the most important factors for a healthy self-
regulation. Several healing factors we find in the communication.
Petzold, Theodor: Errors, Communication… 30.06.2013 -5-
Program Annual PhD Meeting – Thursday, 22 November 2012 Parallel sessions information (2 locations) Parallel sessions A: Big lecture hall (Room 30, Day chair: Laura Koenders) Parallel sessions B: Kapelzaal (Room 16, Day chair: Bernard Bloem) Program 09:00 – 09:45 Registration/ Coffee & Tea 09:45 – 09:55 Welcome by day chair (big lecture hall) 10:00 – 11-30
A Decision Theoretic Cost Model for Dynamic Plans Abstract Since the classic optimization work in System R, query optimization has completely preceded query eval-uation. Unfortunately, errors in cost model parameters such as selectivity estimation compromise the op-timality of query evaluation plans optimized at compile time. The only promising remedy is to interleavestrategy selection and dat
 complex problem, when we try to consider the individual constitution for possible
complications of our treatment decision. Later we will see how shared decision
making helps us in those cases to make less errors or at least errors with less severe
But first we will take it as simple as many people (even health-professionals) see it:
There are streptococcus A as the cause of sore throat and scarlet fever with
sometimes rheumatic endocarditis etc. We can fight these bacteria with penicillin
and evaluate the outcome. The positive effect is about 70 %. Here is not the place to
discuss the outcome in detail compared with other antibiotics. I take this only as an
example to illustrate a very (may be the most) common way to think about causal
medical treatment of diseases. Summing up, it may be said, that a common way of
medical statistical logic takes this way: First you have to make the right disease
diagnosis, than you have to find the means against this disease and at last you hope
This way of medical procedure we can call a "short circuit decision making"
analogous to the electric short circuit, because it uses the very short cut from disease
diagnosis to the treatment - like a computer can do it - without observing the
patients conditions. Most of research is done in this 'short circuit treatment' and
their results we find in the EBM and in the number needed to treat NNT.
May be, that we can recognize the level of systemic errors by looking at the number
needed to treat NNT. The NNT shows us that a treatment benefit for one person
costs the harm of other persons (adverse effects, material costs). So the benefit for
one person statistically depends on the errors in the treatment of several other
persons. The NNT by hypertension with a beta-blocker or … is posed with 86 by an
outcome of a longer life, and 35 by an outcome of a stroke (…??). So - looking for a
longer life - 85 people have to take the medicine in vain therefore one is a winner.
About 13 patients of the 86 suffer about side-effects of the medicine. So the NNT
gives us an idea of systemic errors in treatment of hypertension. Under
the 1st criterion we have about 13 errors and 2-3 hits (included the fewer
strokes). Under the 2nd criterion we find nearly only hits (the symptom of
high blood pressure disappears) and the same under the 3rd.
For example it is obvious in the case of hypertension or a tumour, that disappears by
medical treatment resp. after operation and chemo-therapy, and in contrast the
patient may suffer from the side effects of the treatment more than from the
Petzold, Theodor: Errors, Communication… 30.06.2013 -2-
complex problem, when we try to consider the individual constitution for possible
complications of our treatment decision. Later we will see how shared decision
making helps us in those cases to make less errors or at least errors with less severe
But first we will take it as simple as many people (even health-professionals) see it:
There are streptococcus A as the cause of sore throat and scarlet fever with
sometimes rheumatic endocarditis etc. We can fight these bacteria with penicillin
and evaluate the outcome. The positive effect is about 70 %. Here is not the place to
discuss the outcome in detail compared with other antibiotics. I take this only as an
example to illustrate a very (may be the most) common way to think about causal
medical treatment of diseases. Summing up, it may be said, that a common way of
medical statistical logic takes this way: First you have to make the right disease
diagnosis, than you have to find the means against this disease and at last you hope
This way of medical procedure we can call a "short circuit decision making"
analogous to the electric short circuit, because it uses the very short cut from disease
diagnosis to the treatment - like a computer can do it - without observing the
patients conditions. Most of research is done in this 'short circuit treatment' and
their results we find in the EBM and in the number needed to treat NNT.
May be, that we can recognize the level of systemic errors by looking at the number
needed to treat NNT. The NNT shows us that a treatment benefit for one person
costs the harm of other persons (adverse effects, material costs). So the benefit for
one person statistically depends on the errors in the treatment of several other
persons. The NNT by hypertension with a beta-blocker or … is posed with 86 by an
outcome of a longer life, and 35 by an outcome of a stroke (…??). So - looking for a
longer life - 85 people have to take the medicine in vain therefore one is a winner.
About 13 patients of the 86 suffer about side-effects of the medicine. So the NNT
gives us an idea of systemic errors in treatment of hypertension. Under
the 1st criterion we have about 13 errors and 2-3 hits (included the fewer
strokes). Under the 2nd criterion we find nearly only hits (the symptom of
high blood pressure disappears) and the same under the 3rd.
For example it is obvious in the case of hypertension or a tumour, that disappears by
medical treatment resp. after operation and chemo-therapy, and in contrast the
patient may suffer from the side effects of the treatment more than from the
Petzold, Theodor: Errors, Communication… 30.06.2013 -2-
 Do we need a new strategy for more complex cases?
Do we need a new strategy for more complex cases? 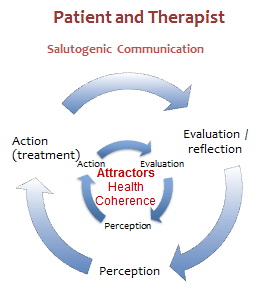 So many patients have made already good and bad experiences with different
diseases and treatments. At last they have to take the medicine, or to walk, or to eat
diet… So we have to bear in mind their self-regulation, their wishes and resources.
The same feedback-loop of communicative self-regulation is active in all systems and
dimensions of life, the physical/somatic, social/emotional, the cultural/mental and
the global/universal/spiritual dimensions.
Regarding the theme of this conference: when we recognize the discrepancy
between our medical aim of healthiness and the huge number of 'adverse events' we
begin to learn - remembering our attractive aim.
So the required strategy for treating patients suffering of more complex conditions
focuses the healthy self-regulation and strives to stimulate and promote it. Diseases
and illnesses are not seen any longer as separable entities but as dynamical
interactive processes of human beings, which we desire to progress in direction of
Therapists accompany patients during their self-regulated healthy
development by communication. At first they reflect and evaluate why the patient
needs help (anamnesis). Then they perceive the actual state (self-perception and
examination by the doctor). In the next phase they look for the resources they have
for treatment, for managing the next step towards health and make a shared
decision. At last in the consultation you can already make an evaluation by imaging
the result of your action resp. treatment. At the next appointment you will do the
How we can learn from errors quickly and minimize severe
So many patients have made already good and bad experiences with different
diseases and treatments. At last they have to take the medicine, or to walk, or to eat
diet… So we have to bear in mind their self-regulation, their wishes and resources.
The same feedback-loop of communicative self-regulation is active in all systems and
dimensions of life, the physical/somatic, social/emotional, the cultural/mental and
the global/universal/spiritual dimensions.
Regarding the theme of this conference: when we recognize the discrepancy
between our medical aim of healthiness and the huge number of 'adverse events' we
begin to learn - remembering our attractive aim.
So the required strategy for treating patients suffering of more complex conditions
focuses the healthy self-regulation and strives to stimulate and promote it. Diseases
and illnesses are not seen any longer as separable entities but as dynamical
interactive processes of human beings, which we desire to progress in direction of
Therapists accompany patients during their self-regulated healthy
development by communication. At first they reflect and evaluate why the patient
needs help (anamnesis). Then they perceive the actual state (self-perception and
examination by the doctor). In the next phase they look for the resources they have
for treatment, for managing the next step towards health and make a shared
decision. At last in the consultation you can already make an evaluation by imaging
the result of your action resp. treatment. At the next appointment you will do the
How we can learn from errors quickly and minimize severe