L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Prostata-shg-bretten.de
P r o s t a t e C a n c e r D N A P l o i d y a n d R e s p o n s e t o S a l v a g e H o r m o n e T h e r a p y A f t e r R a d i o t h e r a p y W i t h o r W i t h o u t S h o r t - T e r m T o t a l A n d r o g e n B l o c k a d e : A n A n a l y s i s o f R T O G 8 6 1 0
By A. Pollack, D.J. Grignon, K.H. Heydon, E.H. Hammond, C.A. Lawton, J.B. Mesic, K.K. Fu, A.T. Porter,
Purpose: DNA ploidy has consistently been found to be a Results: DNA nondiploidy was not associated with any correlate of prostate cancer patient outcome. However, a of the other prognostic factors in univariate analyses. In minority of studies have used pretreatment diagnostic ma- Kaplan-Meier analyses, 5-year overall survival was 70% terial and have involved radiotherapy (RT)-treated patients. for those with diploid tumors and 42% for nondiploid tu- In this retrospective study, the predictive value of DNA mors. Cox proportional hazards regression revealed that ploidy was evaluated in patients entered into Radiation nondiploidy was independently associated with reduced Therapy Oncology Group protocol 8610. The protocol treat- overall survival. No correlation was observed between ment randomization was RT alone versus RT plus short- DNA ploidy and distant metastasis. The diminished survival course (ϳ4 months) neoadjuvant and concurrent total an- in the absence of an increase in distant metastasis was drogen blockade (RT؉TAB). related to a reduction in the effect of salvage androgen Patients and Methods: The study population consisted of ablation; patients treated initially with RT؉TAB and who 149 patients, of whom 74 received RT alone and 75 re- had nondiploid tumors had reduced survival after salvage ceived RT؉TAB. DNA content was determined by image androgen ablation. analysis of Feulgen stained tissue sections; 94 patients were Conclusions: Nondiploidy was associated with shorter diploid and 55 patients were nondiploid. Kaplan-Meier survival, which seemed to be related to reduced response to univariate survival, the cumulative incidence method, and salvage hormone therapy for those previously exposed to Cox proportional hazards multivariate analyses were used short-term TAB. to evaluate the relationship of DNA ploidy to distant metas- J Clin Oncol 21:1238-1248. 2003 by American tasis and overall survival. Society of Clinical Oncology.
DNA PLOIDY has been investigated as a potential prognos- characterized in the diagnostic material from patients participating
tic factor for prostate cancer for many years, and in the
in Radiation Therapy Oncology Group (RTOG) protocol 8610.27
vast majority of reports, it has been found to be predictive of
RTOG protocol 8610 was a phase III randomized clinical trial
patient outcome.1-20 However, most of these studies were done
designed to assess the effect of RT plus short-term neoadjuvant
using tissue from prostatectomy specimens. Far fewer have
and concurrent total androgen blockade (RTϩTAB) as com-
examined DNA ploidy as a pretreatment correlate of patient
pared with RT alone. The patients enrolled had locally advanced
outcome using diagnostic material. Moreover, there are few
disease; tumors had a palpable surface area of 25 cm2 or greater.
reports wherein the predictive value of DNA ploidy was inves-
In addition, nearly one third of the patients had Gleason score 8
tigated in prostate cancer patients treated with definitive radio-
to 10 disease and 8% had documented lymph node involve-ment.27 The purpose of this analysis was to assess the prognostic
therapy (RT). Conclusions about the association of DNA ploidy
significance of DNA ploidy, as determined by image analysis,
with outcome after RT are unclear because the findings have
for prostate cancer patients with high-risk features and to
been somewhat divergent.21-26 In this analysis, DNA ploidy was
determine whether the addition of androgen ablation to RTaffected the prognostic value of these measurements. There were456 evaluable patients entered into the trial, and of these, 149
From the Department of Radiation Oncology, Fox Chase Cancer Center,
(33%) had tissue available for DNA ploidy analysis. These
and Radiation Therapy Oncology Group, Philadelphia, PA; Department of
patients are the subjects of this report. Pathology, Karmanos CA Institute, and Department of Radiation Oncology,Wayne State University, Detroit, MI; Radiation Therapy Oncology Group,Philadelphia, PA; Department of Pathology, LDS Hospital, Salt Lake City,Utah; Department of Radiation Oncology, Medical College of Wisconsin,Milwaukee, WI; Radiation Oncology Center, Sacramento; and Departmentof Radiation Oncology, University of California, San Francisco, CA;
The study population included patients entered into RTOG protocol 8610,
Division of Radiation Oncology, Johns Hopkins Hospital, Baltimore, MD;
entitled "A phase III trial of Zoladex and flutamide used as cytoreductive
and Department of Radiation Oncology, Massachusetts General Hospital,
agents in locally advanced carcinoma of the prostate treated with definitive
radiotherapy."27 This phase III randomized clinical trial for locally advanced
Submitted February 8, 2002; accepted December 18, 2002.
prostate cancer was closed in 1991 and accrued a total of 471 patients, 456
Address reprint requests to Alan Pollack, MD, PhD, Department of
of whom were evaluable. TAB with flutamide and goserelin acetate (Zola-
Radiation Oncology, Fox Chase Cancer Center, 7701 Burholme Ave,
dex) was given for a total of 4 months, starting 2 months before radiotherapy
Philadelphia, PA 19111; email: A_Pollack@FCCC.edu. 2003 by American Society of Clinical Oncology.
Tissue blocks were obtained from 261 (57%) of the 456 evaluable patients.
After hematoxylin- and eosin-stained samples were sectioned and reviewed,
Journal of Clinical Oncology, Vol 21, No 7 (April 1), 2003: pp 1238-1248
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Table 1. Pretreatment Characteristics Table 2. Potential Pretreatment Predictors of 5-Year* Distant Metastasis, Any Failure, and Overall Survival (n ؍ 456†)
Abbreviations: DM, distant metastasis; AF, any failure; OS, overall survival; NA,
not analyzed; RT, radiotherapy; TAB, total androgen blockade.
*Kaplan-Meier analysis and log-rank test for AF (including death) and OS.
Cumulative incidence and Gray's test for DM.
†There are 429 patients with Gleason score, 149 with DNA-ploidy, and 129 with
Abbreviations: KPS, Karnofsky performance status; RT, radiotherapy; TAB, total
androgen blockade; NS, not significant.
(Sunnyvale, CA) mounted on an Olympus BH-2 microscope (Lake Success,
NY) and a Sony monitor (San Jose, CA) were used to scan the specimens.
†Those with unknown p53 were not included in the analysis.
For each sample, tumor cell and control cell nuclei were taken from the
same slide. Each area of interest in the tissue was designated on the slideusing a marking pen. For each slide, a black level and incident light levelwere set for calibration. Each designated area was scanned from left to right
sufficient tumor for DNA ploidy analysis was present in 149 patient samples.
covering each field only once. Nuclei were chosen because they appeared not
The diagnostic material, which consisted of 113 samples from needle
to be overlapped by other nuclei. For each sample, 100 control nuclei
biopsies and 36 samples from transurethral resectates, was requested from
(endogenous fibroblasts) and 200 tumor nuclei were measured. The DNA
participating institutions (Ͼ 100), reviewed centrally by the study pathologist
content was plotted as Feulgen-stained DNA versus cell number and
(D.J. Grignon) in 98% of cases, and graded according to Gleason.28 A global
displayed in histograms. The DNA content mean, SD, and coefficient of
Gleason score was assigned. The distribution of patients by Gleason score for
variation (CV) were calculated for the control cells (2C control). The mean
the study group was 22 in Gleason score 2 to 5, 16 in Gleason score 6, 60 in
was used to calculate the DNA index (DI), which was the ratio of the mean
Gleason score 7, and 50 in Gleason score 8 to 10; one patient case was not
nuclear cell DNA content of tumor population divided by the mean of the 2C
graded. The distribution of patients by clinical T category was 38 in T2 and
111 in T3. At the time the trial was initiated, pretreatment prostate-specific
Tumor nuclei populations were considered diploid if the main peak DI was
antigen (PSA) was not routinely used in the clinic. Pretreatment serum PSA
0.80 to 1.20 with less than 35% of other DNA measurements outside of 2C
values were available for only 19 (15%) patients of the study cohort and, as
ϩ 2SD (on the basis of the control nuclei population). Populations were
a consequence, are not included in the statistical analyses. A prior immuno-
considered aneuploid if the main peak DI was less than 0.80 (hypodiploid) or
histochemical analysis of p53 status was done in 129 patients29 who
greater than 1.20 (hyperdiploid) and were not considered tetraploid. Tet-
participated in RTOG protocol 8610. In that report, abnormal p53 expression
raploid populations had a DNA index of 1.80 to 2.20. Patients who had
(p53-positive by immunohistochemistry) was found to be significantly
multiple peaks were considered aneuploid if more than 35% of the tumor
correlated with reduced survival. For this reason, p53 status is included in the
nuclei population formed peaks in the range greater than 2C Ϯ 2SD.
analysis here. p53 status and DNA ploidy were determined in 113 patients. DNA Content Measurements by Image Analysis
The end points used in the analysis were distant metastasis, any failure,
For inclusion in the study, the stained section had to contain identifiable
and overall survival. The parameters of distant metastasis and overall
carcinoma. Sections were evaluated without knowledge of patient outcome.
survival are as described in the initial report.27 PSA, or biochemical, failure
Sections cut 6 m thick on poly-L slides from paraffin-embedded formalin-
was included in the definition of any failure. The original treatment protocol
fixed tissues were deparaffinized in xylene and rehydrated in a series of
was designed before the increasing PSA profile was established as an end
ethanol washes (100%, 95%) to a final distilled water step. Slides were then
point. Consequently, a PSA of more than 1.5 ng/mL 1 year after random-
placed in 5 N HCl for 60 minutes, stained with Schiff's reagent for 60
ization was used as an approximation of biochemical failure. Five patients
minutes, rinsed in a sodium metabisulfite rinse (10% Na S O in 1 N HC1),
died before 1 year, and 11 other patients did not have posttreatment PSA data
dehydrated in reagent alcohol, and then cleared in xylene. Coverslips were
for determining biochemical failure; these patients were excluded from the
added to slides using synthetic mounting media.
analysis of this end point. Local and regional failures were also included in
Measurements were obtained at ϫ200 magnification using 560-nm mono-
the definition of any failure. Local failure was defined as an increase in tumor
chromatic light. DNA quantification was performed using the Image Measure
size of more than 50% for patients in whom complete tumor regression did
software program (Phoenix Technology, Inc, Seattle, WA), with a PCVision
not occur or as recurrence of a palpable nodule when there was complete
Plus digitizing frame-grabber board (Imaging Technology, Inc, Woburn, MA)
regression or a positive biopsy of the prostate after 2 or more years of
and a Logitech mouse (Fremont, CA). Both a Pulnix TM-745 camera
follow-up. Regional metastasis included clinical or radiologic evidence of
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Fig 1. Kaplan-Meier survival analysis of overall sur- vival (upper) and distant failure (lower) for patients with diploid (--) and nondiploid tumors (- - - -). The tic marks represent the times at which patients were censored, and the numbers of patients at risk are displayed above the x-axis.
disease in the pelvis other than in the prostate. Distant metastasis was defined
The distributions of patient characteristics and treatment assignments were
as clinical or radiologic evidence of disease outside the pelvis. Any failure
compared by the Pearson 2 test with the Yates correction factor. Overall
was defined as first reported failure, local failure (n ϭ 9), regional failure
survival and any failure estimates were derived using the Kaplan-Meier
(n ϭ 0), distant failure (n ϭ 11), local plus distant failure (n ϭ 11), biochemical
method.30 Gelman et al31 and Gaynor et al32 indicated in their respective
failure (n ϭ 112), or death (n ϭ 0). All end points, with the exception of
papers that the Kaplan-Meier method generally overestimates distant metas-
biochemical failure, were measured from the date of randomization to the first
tasis. The cumulative incidence approach was used instead to estimate distant
reported failure date or last follow-up date in the absence of failure. The
metastasis because it specifically adjusts for competing risk such as dying
biochemical failure end point started 1 year after randomization.
without recurrence of prostate cancer.33 Univariate comparisons of overallsurvival and any failure were calculated with the log-rank test.34 Univariate
comparisons of local failure, distant failure, and biochemical failure were
The published analysis of the evaluable patients on the trial was performed
on 456 patients. The current analysis was done on 149 patients, with the
Multivariate Cox proportional hazard models were applied to each of the
potential for an additional 6 years of follow-up, as compared with the initial
three end points. The initial multivariate analyses were restricted to only
treatment report.27 As of June 30, 2000, the median follow-up of the alive
patients who had DNA ploidy determination. The analyses determined
patients in the study cohort was 9 years (range, 1.2 to 11.8 years).
whether DNA content was of prognostic value after adjusting for treatment
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 2. Kaplan-Meier analysis of overall survival for patients randomly assigned to RT alone (upper) or RT؉TAB (lower) when subdivided by DNA ploidy status of diploid (solid line) and nondiploid (- - - -). The tic marks represent the times at which patients were censored, and the num- bers of patients at risk are displayed above the x-axis.
assignment and Gleason score as fixed covariates.36 All factors were
ploidy determinations, and 129 (28%) had p53 determinations. In only 113
considered as dichotomous variables and coded as follows: treatment
(25%) patients were both ploidy and p53 determinations available. There are
assignment (0 for RT alone v 1 for RT ϩ hormones), grouped Gleason sums
potential problems caused by the missing values. Selection bias may occur,
(0 for sums 2 to 6 v 1 for sums 7 to 10), p53 (0 for negative v 1 for positive),
wherein the patients in whom the assays were done do not constitute a
and DNA content (0 for diploid v 1 for nondiploid). The fitted parameter
random sample from the whole study. Consequently, the study cohort may
from the Cox model was used to estimate the relative risk associated with
have a better or worse outcome than the parent cohort. Moreover, when
each prognostic variable and the corresponding 95% confidence interval. A
patients with missing values are excluded in the analysis, the number of
ratio of 1 would indicate no difference between the two subgroups. The
patients to be analyzed may be relatively small, compromising the statistical
larger the difference from 1, the greater the difference in the failure rates
power needed to detect clinically meaningful differences.
between the two subgroups. The treatment effect was modeled in such a way
To adjust for the problem of missing values in the second multivariate
that a value less than 1 favored the addition of hormones. DNA ploidy was
analysis, two variables instead of one were used to evaluate each marker. For
modeled in a way that a value greater than 1 indicates a greater risk of failure
DNA ploidy, patients were divided into three categories: determination not
for DNA nondiploidy. All of the statistical comparisons were made with
done, diploid, and nondiploid. For p53, patients were divided into three
categories: determination not done, negative, and positive. The first variable
Another multivariate analysis adjusted for two additional factors: p53 and
for DNA ploidy would then be 0 for diploid/not done versus 1 for nondiploid,
missing tumor determinations. Of the 456 evaluable patients, 149 (33%) had
and the second variable would be 0 for nondiploid/not done versus 1 for
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Table 3. Cox Proportional Hazards Regression Analyses (n ؍ 149)*
Abbreviations: RR, relative risk; CI, confidence interval; DM, distant metastasis; AF, any failure (including death); OS, overall survival; NA, not analyzed; RT, radiotherapy;
*The analysis was performed on 149 patients, in whom all factors were present. p53 status was not included.
diploid. The estimated relative risk of DNA ploidy was figuratively obtained by
differences in the distribution of patients between the diploid and
subtracting out the two variables. The 27 patients without centrally reviewed
nondiploid groups, although a borderline significant relationship
Gleason scores were excluded, leaving 429 patients for the analysis.
was seen with Gleason score. Of those that were nondiploid,
83% had a Gleason score of 7 to 10, as opposed to 69% for thosethat were diploid (P ϭ.057). In a prior analysis of this patient
On the basis of DNA content measurement, 94 patients were
cohort,29 abnormal p53 expression was reported to be a signif-
classified as diploid, nine patients were classified as tetraploid,
icant correlate of decreased overall survival and so is included
and 46 patients were classified as aneuploid. Because the number
here. There was no association between the distribution of patients
of tetraploid patients was small and not amenable to separate
by p53 status and DNA ploidy (correlation coefficient ϭ 0.05).
analysis, the nondiploid patients (tetraploid plus aneuploid;
Five-year Kaplan-Meier estimates of overall survival and any
n ϭ 55) were pooled, as has been described previously.22 Table
failure rates for all patients with the listed variable are shown in
1 shows the distribution of patients by pretreatment characteris-
Table 2. Five-year estimates of distant failure rates derived using
tics and DNA ploidy. There were no statistically significant
the cumulative incidence method are also shown in Table 2. Allfactors listed in the table, including DNA ploidy, affected overall
Table 4. Characteristics of Patients Who were Entered in RTOG 8610 by
survival (assigned treatment and p53 status were borderline). Presence or Absence of Ploidy Data
Estimated 5-year overall survival was only 42% when nondip-
loidy was present, versus 70% in diploid patients (Fig 1). Figure
2 shows the breakdown of overall survival rates by protocol
treatment assignment and DNA ploidy. Reduced survival rates
were observed with nondiploidy in both treatment groups, but
the difference between diploid and nondiploid only reached signif-
RTOG protocol 8610 had advanced disease, and this is reflected in
the high failure of any type and low overall survival rates. Although
the main end point of the study was overall survival, the other end
points shed light into how survival was affected.
Gleason score, assigned treatment on protocol, and p53 status
were associated with all of the end points shown in Table 2.
These associations demonstrate a logical relationship between
progression, distant metastasis, and overall survival. Such a
pattern, however, was not discerned for DNA ploidy in univariate or
Table 5. Univariate Analysis of Outcome by Whether DNA Ploidy Determination Was or Was Not Done
Abbreviations: RTOG, Radiation Therapy Oncology Group; KPS, Karnofsky
performance status; RT, radiotherapy; TAB, total androgen blockade; NS, not
†Those with unknown p53 were not included in this analysis.
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Table 6. Adjusted Cox Proportional Hazards Regression Analyses (n ؍ 429)
Abbreviations: RR, relative risk; CI, confidence interval; DM, distant metastasis; AF, any failure (including death); OS, overall survival; NA, not analyzed; RT, radiotherapy;
Cox proportional hazards regression analyses. Survival was worse
DNA ploidy was related to overall survival in multivariate
when DNA nondiploidy was found, whereas any failure and distant
analysis, yet no association with distant metastasis was observed.
metastasis rates were not related to ploidy status.
From these data, it is not intuitive how DNA ploidy affected
The initial multivariate analyses were performed using the 149
survival. The lack of a significant correlation between nondip-
patients with a DNA ploidy determination. DNA ploidy was
loidy and distant metastasis, although reduced survival was
associated with overall survival after controlling for assigned
evidenced, led us to examine survival after the institution of
treatment and Gleason score (Table 3). When this subset was
salvage hormone therapy. Figure 3 shows that overall survival at
compared with the parent cohort, the differences in baseline
5 years after salvage hormone therapy was significantly lower in
characteristics were marginal (Table 4), whereas the differences
the presence of nondiploidy (45% v 23%; P ϭ.018). Because the
in patient outcome were highly significant (Table 5). For
difference in overall survival could be related to an imbalance of
example, patients with a DNA ploidy determination had an
intercurrent deaths, disease-specific survival results were
increased risk of death and any failure. In a previously reported
compared. Even though there were fewer patients available
analysis, p53 status was found to be a significant prognostic
for the analysis of disease-specific survival (n ϭ 40), and
variable for survival but was only available for 113 patients with
therefore power was reduced, a borderline significant trend
a DNA ploidy determination. As a consequence, a multivariate
favoring the diploid population was observed (63% v 25% at
analysis that adjusted for this population selection effect was
3 years; P ϭ.06). The disease-specific survival results mirror
done using 429 patients (see Methods). Table 6 shows that after
adjusting for population effects and p53 status, in addition to
Figure 4 indicates that the reduced survival of nondiploidy
Gleason score and assigned treatment, DNA ploidy was an
patients after salvage hormone therapy was the result of salvage
independent prognostic factor for overall survival.
hormone therapy resistance of these patients when they were
Fig 3. Kaplan-Meier analysis of overall survival after salvage hormone therapy was started for patients with diploid (--) and nondiploid tumors (- - - -). The tic marks represent the times at which patients were censored, and the numbers of patients at risk are displayed above the x-axis.
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Fig 4. Kaplan-Meier analysis of overall survival after salvage hormone therapy (HT) by the treatment random- ization of RT alone (upper) and RT؉TAB (lower) when subdivided by DNA ploidy status of diploid (--) and nondiploid (- - - -). The tic marks represent the times at which patients were censored, and the numbers of pa- tients at risk are displayed above the x-axis.
assigned randomly to RTϩTAB. This apparent resistance might
absolute rate of distant metastasis that translated into reduced
be explained by an unequal distribution of patients with distant
survival, but probably more rapid progression to death once
metastasis at the time salvage hormone therapy was initiated.
distant metastasis was discernible. Prior treatment with TAB in
Figure 5 shows that the same pattern was observed for
nondiploid patients may promote resistance to salvage hormone
RTϩTAB-treated patients who did not have evidence of distant
therapy, thereby shortening survival.
metastasis at the start of salvage hormone therapy. Overall
Other potential DNA ploidy-associated differences in treat-
survival at 5 years for patients who had distant metastasis at the
ment outcome based on the protocol treatment assignments of
time of salvage hormone therapy was 15% (n ϭ 14) for patients
RT alone versus RTϩTAB are explored in Table 7. In general,
randomly assigned to RT alone and 11% (n ϭ 10) for those
failure rates were more significantly reduced by RTϩTAB
randomly assigned to RTϩTAB. Subdivision by DNA ploidy
compared with RT alone for those with diploid tumors than for
had no effect on these relationships.
those with nondiploid tumors. These results combined with the
Figure 6 is an analysis of time to distant metastasis after
findings that survival after salvage hormone therapy is shortened
salvage hormone therapy for patients who were free of distant
indicate that short-term adjuvant TAB is not advisable in the
metastasis at that time. The results indicate that it is not the
presence of nondiploidy. Such subgroup analyses are fraught
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 5. Kaplan-Meier analysis of overall survival after salvage hormone therapy (HT) when distant metastasis (DM) is absent. The patients are categorized by the treat- ment randomization of RT alone (upper) and RT؉TAB (lower) as subdivided by DNA ploidy status of diploid (- - - -) and nondiploid (--). The tic marks represent the times at which patients were censored, and the numbers of patients at risk are displayed above the x-axis.
with potential errors related to the influence of unevenly distrib-
loidy.37 However, DNA ploidy analysis has not established a
uted prognostic factors. Nonetheless, the results support consid-
foothold in clinical practice. One explanation is that the majority
eration of DNA ploidy analysis in future trials of short-term
of prior studies have not analyzed diagnostic material.
For patients managed by RT, only a handful of reports have
examined the association of DNA ploidy with outcome.21-26
Although the results have not been entirely consistent, nondip-
Pretreatment prognostic factors have proven valuable in de-
loidy has been related to poor patient outcome in the majority of
termining prostate cancer patient treatment strategies, especially
studies. These reports have involved relatively small numbers of
in defining patients who should receive androgen ablation in
patients, and additional characterizations of DNA ploidy as a
combination with RT. The core factors used in clinical practice
prognostic factor are needed. To our knowledge, no reports have
are serum PSA, Gleason score, and clinical stage.37 Apart from
described the predictive value of DNA ploidy for patients
these, and possibly the proportion of cancer in the biopsy
specimens,38 the most widely investigated and promising marker
The data presented revealed a number of relationships be-
of disease progression and reduced survival is DNA nondip-
tween DNA ploidy and patient outcome. For the multivariate
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
Fig 6. Kaplan-Meier analysis of the relationship of DNA ploidy to distant failure after salvage hormone ther- apy (HT) when distant metastasis (DM) was absent. This analysis was restricted to patients randomly assigned to RT؉TAB. The tic marks represent the times at which pa- tients were censored, and the numbers of patients at risk are displayed above the x-axis.
analyses using the 149 patients with DNA ploidy determinations
distant metastasis. DNA nondiploidy, in this locally advanced
(Table 3) or the adjusted analyses using the 429 patients
high-risk cohort, was not a predictor of distant metastasis.
available from the entire cohort (Table 6), nondiploidy was
DNA nondiploidy has been correlated with reduced prostate
associated with reduced overall survival without any increase in
cancer patient survival in numerous reports.37 This correlation
distant metastasis. In other studies, nondiploidy consistently has
was also observed in the data presented here, despite the lack of
been a robust correlate of clinical disease progression (local,
a relationship between nondiploidy and distant metastasis. The
regional, and distant). Few examples exist in which distant
results in Fig 3 indicate that DNA ploidy was associated with
metastasis has been analyzed separately,5,22 but there is every
survival because the nondiploid cases progressed to death more
indication that nondiploidy is related to more rapid progression
rapidly after the initiation of salvage hormone therapy. On
to distant metastasis and that survival is, therefore, reduced.
further examination, the nondiploid patients who were initially
The prostate cancer patient population studied in RTOG
treated with RTϩTAB were dramatically more resistant to
protocol 8610 was clearly locally advanced and not typical of
androgen ablation salvage (Fig 4). Short-term adjuvant TAB,
those treated with RT today. Overall, biochemical failure was
combined with RT, could have predisposed patients to resistance
78% at 5 years, indicating that the treatments used were
to salvage hormone therapy. Although others have shown that
inadequate. This biochemical failure rate translated into a 36%
response to androgen ablation is less pronounced when DNA
distant metastasis rate. The rates of distant metastasis in the
nondiploidy is identified,39-43 this is the first description that
presence of diploidy and nondiploidy were 35% and 39%,
adjuvant androgen ablation in such cases may predispose pa-
respectively, which were not different statistically in univariate
tients to resistance to androgen ablation salvage.
or multivariate analyses. Because the number of patients exhib-
The data presented, however, are not conclusive for a number
iting distant failures was 46 of 94 and 22 of 55 for the diploid
of reasons. First, there was no evidence of an increased rate of
and nondiploid cases, respectively, there were sufficient events
distant metastasis in those with nondiploidy. The compromised
to measure the effect of DNA ploidy. In multivariate analysis,
survival rate of nondiploid patients treated with RTϩTAB after
p53 status and Gleason score were independent correlates of
salvage hormone therapy seemed to be independent of distantmetastasis rates (Fig 6). Second, Shipley et al44 recently pre-sented an analysis of this type for the entire group of patients in
Table 7. Relationship of DNA Ploidy Stratified by Study Randomization to
RTOG protocol 8610, and they did not find a statistically
Patient Outcome
significant difference in survival after salvage hormone therapy
based on assigned treatment (RT alone v RTϩTAB). Likewise,
for the DNA-ploidy cohort studied here, there was no difference
in survival after salvage hormone therapy based on assigned
treatment (data not shown). However, as shown in Fig 4, survival
was reduced for patients who had nondiploidy and who were
ϩTAB. Therefore, patients with diploidy who
were assigned to RTϩTAB should have had a better survival
Abbreviations: RT, radiotherapy; TAB, total androgen blockade; DM, distant
than those assigned to RT alone. A nonsignificant trend in this
metastasis; AF, any failure; OS, overall survival.
*Log-rank test for AF and OS; Gray's test DM.
direction was observed wherein the survival of diploid patients
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
treated with RTϩTAB after salvage hormone therapy was higher
prostate DNA ploidy status,12,45,46 which may be measured on
than for those treated with RT alone (55% v 39%; P ϭ.54). This
thin sections using image analysis. The image analysis technique
may have contributed to the difference in survival between
for quantifying DNA content used in this report is the preferred
diploidy and nondiploidy for those treated with RTϩTAB.
method for the analysis of DNA ploidy status in diagnostic
Third, although the cause of death is not always clear for prostate
needle biopsy specimens because it requires less tissue than flow
cancer patients receiving salvage therapy, there was a slightly
cytometry and allows for the histologic separation of normal
greater proportion of intercurrent deaths in those with nondip-
epithelial and stromal cells from diploid tumor cells (a problem
loidy (46%) compared with those with diploidy (39%). Despite
that plagues flow cytometric analyses). The data presented show
these potentially complicating factors, the overriding concern
that locally advanced patients with nondiploidy have reduced
raised by the findings is that short-term neoadjuvant or adjuvant
survival. The most striking association was that RT plus short-
TAB may promote resistance to salvage hormone therapy and more
term neoadjuvant and concurrent TAB may predispose patients
rapid progression to death once distant metastasis has occurred. This
with nondiploidy to reduced survival after salvage hormone
hypothesis needs to be confirmed in another group of patients.
therapy. As with all retrospective tumor marker studies, this is a
In conclusion, DNA ploidy shows promise in predicting the
subset analysis, and although we attempted to correct for
outcome of prostate cancer patients. Few reports exist on the
selection bias, it is possible that the findings are not representa-
relationship of DNA ploidy to outcome after RT, although there
tive. One should consider, however, that these data are consistent
is ample evidence that nondiploidy is an independent adverse
with prior reports that affirm the independent merit of DNA
factor that should be considered in treatment planning. Pretreat-
ploidy. DNA ploidy will likely become an important factor for
ment diagnostic material provides a reasonable representation of
the stratification of patients in future trials.
1. Fordham MVP, Burdget AH, Matthews J, et al: Prostatic carcinoma
15. Hawkins CA, Bergstralh EJ, Lieber MM, et al: Influence of DNA
cell DNA content measured by flow cytometry and its relation to clinical
ploidy and adjuvant treatment on progression and survival in patients with
pathologic stage T3 (PT3) prostate cancer after radical prostatectomy.
2. Lee SE, Currin SM, Paulson DF, et al: Flow cytometric determination
of ploidy in prostatic adenocarcinoma: A comparison with seminal vesicle
16. Di Silverio F, D'Eramo G, Buscarini M, et al: DNA ploidy, Gleason
involvement and histopathological grading as a predictor of clinical recur-
score, pathological stage and serum PSA levels as predictors of disease-free
survival in C-D1 prostatic cancer patients submitted to radical prostatectomy.
3. Winkler HZ, Rainwater LM, Myers RP, et al: Stage D1 prostatic
adenocarcinoma: Significance of nuclear DNA ploidy patterns studied by
17. Ahlgren G, Lindholm K, Falkmer U, et al: A DNA cytometric
flow cytometry. Mayo Clin Proc 63:103-112, 1988
proliferation index improves the value of the DNA ploidy pattern as a
4. Nativ O, Winkler HZ, Raz Y, et al: Stage C prostatic adenocarcinoma:
prognosticating tool in patients with carcinoma of the prostate. Urology
Flow cytometric nuclear DNA ploidy analysis. Mayo Clin Proc 64:911-919,
18. Amling CL, Lerner SE, Martin SK, et al: Deoxyribonucleic acid
5. Adolfsson J, Ro¨nstro¨m L, Hedlund P-O, et al: The prognostic value of
ploidy and serum prostate specific antigen predict outcome following salvage
modal deoxyribonucleic acid in low grade, low state untreated prostate
prostatectomy for radiation refractory prostate cancer. J Urol 161:857-862,
6. Haugen OA, Mjølnerød O: DNA-ploidy as prognostic factor in
19. Diaz JI, Mora LB, Austin PF, et al: Predictability of PSA failure in
prostatic carcinoma. Int J Cancer 45:224-228, 1990
prostate cancer by computerized cytometric assessment of tumoral cell
7. Montgomery BT, Nativ O, Blute ML, et al: Stage B prostate adeno-
carcinoma: Flow cytometric nuclear DNA ploidy analysis. Arch Surg
20. Cheng L, Darson MF, Slezak J, et al: Correlation of margin status and
extraprostatic extension with progression of prostate carcinoma. Cancer
8. Visakorpi T, Kallioniemi O-P, Paronen IYI, et al: Flow cytometric
analysis of DNA ploidy and S-phase fraction from prostatic carcinomas:
21. Song J, Cheng WS, Cupps RE, et al: Nuclear deoxyribonucleic acid
Implications for prognosis and response to endocrine therapy. Br J Cancer
content measured by static cytometry: Important prognostic association for
patients with clinically localized prostate carcinoma treated by external beam
9. Wirth MP, Mu¨ller HA, Mansek A, et al: Value of nuclear DNA ploidy
patterns in patients with prostate cancer after radical prostatectomy. Eur Urol
22. Gauwitz MD, Pollack A, El-Naggar AK, et al: The prognostic
significance of DNA ploidy in clinically localized prostate cancer treated
10. Tinari N, Natoli C, Angelucci D, et al: DNA and S-Phase fraction
with radiation therapy. Int J Radiat Oncol Biol Phys 28:821-828, 1994
analysis by flow cytometry in prostate cancer: Clinicopathologic implica-
23. Centeno BA, Zietman AL, Shipley WU, et al: Flow cytometric
analysis of DNA ploidy, percent S-phase fraction, and total proliferative
11. Blatstein LM, Ginsberg PC, Daskal I, et al: Flow cytometric deter-
fraction as prognostic indicators of local control and survival following
mination of ploidy in prostatic adenocarcinoma and its relation to clinical
radiation therapy for prostate carcinoma. Int J Radiat Oncol Biol Phys
outcome. J Am Osteopath Assoc 93:463-472, 1993
12. Ross JS, Figge H, Bui HX, et al: Prediction of pathologic stage and
24. Pollack A, Zagars GK, El-Naggar A, et al: Near-diploidy: A new
postprostatectomy disease recurrence by DNA ploidy analysis of initial
prognostic factor for clinically localized prostate cancer treated with external
needle biopsy specimens of prostate cancer. Cancer 74:2811-2818, 1994
beam radiotherapy. Cancer 73:1896-1903, 1994
13. Vesalainen S, Nordling S, Lipponen P, et al: Progression and survival
25. Pollack A, Zagars GK, El-Naggar A, et al: Relationship of tumor
in prostatic adenocarcinoma: A comparison of clinical stage, Gleason grade,
DNA-ploidy to serum prostate-specific antigen doubling time after radio-
S-phase fraction and DNA ploidy. Br J Cancer 70:309-314, 1994
therapy for prostate cancer. Urology 44:711-718, 1994
14. Carmichael MJ, Veltri RW, Partin AW, et al: Deoxyribonucleic acid
26. Khoo VS, Pollack A, Cowen D, et al: Relationship of Ki-67 labeling
ploidy analysis as a predictor of recurrence following radical prostatectomy
index to DNA-ploidy, S-phase fraction, and outcome in prostate cancer
for Stage T2 disease. J Urol 153:1015-1019, 1995
treated with radiotherapy. Prostate 41:166-172, 1999
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
27. Pilepich MD, Krall JM, Al-Sarraf M, et al: Androgen deprivation with
38. Iczkowski KA, Bostwick DG: Prostate biopsy interpretation. Current
radiation therapy compared with radiation therapy alone for locally advanced
concepts, 1999. Urol Clin North Am 26:435-452, 1999
prostatic carcinoma: A randomized comparative trial of the Radiation
39. Forsslund G, Zetterberg A: Ploidy level determinations in high grade and low
Therapy Oncology Group. Urology 45:616-623, 1995
grade malignant variants of prostatic carcinoma. Cancer Res 50:4281-4285, 1990
28. Gleason DF: Classification of prostatic carcinomas. Cancer Che-
40. Stege R, Tribukait B, Lundh B, et al: Quantitative estimation of tissue
prostate specific antigen, deoxyribonucleic acid ploidy and cytological grade
29. Grignon D, Caplan R, Sarkar FH, et al: P53 status and prognosis of
in fine needle aspiration biopsies for prognosis of hormonally treated
locally advanced prostatic adenocarcinoma: A study based on RTOG 8610.
prostatic carcinoma. J Urol 148:833-837, 1992
41. Forsslund G, Nilsson B, Zetterberg A: Near tetraploid prostate
30. Kaplan EL, Meier P: Nonparametric estimation from incomplete
observations. J Am Stat Assoc 53:457-481, 1958
42. Pollack A, Troncoso P, Zagars GK, et al: The significance of
31. Gelman R, Gelber R, Henderson IC, et al: Improved methodology for
DNA-ploidy and S-phase fraction in node-positive (Stage D1) prostate
analyzing local and distant recurrence. J Clin Oncol 8:548-555, 1990
cancer treated with androgen ablation. Prostate 31:21-28, 1997
32. Gaynor JJ, Feuer EJ, Tan CC, et al: On the use of cause-specific
43. Seay TM, Blute ML, Zincke H: Long term outcome in patients with
failure and conditional failure probabilities: Example from clinical oncology
pTxNϩ adenocarcinoma of the prostate treated with radical prostatectomy
and early androgen ablation. J Urol 159:357-364, 1998
33. Kalbfleisch JD, Prentice RL. The Statistical Analysis of Failure Time
44. Shipley WU, Lu JD, Pilepich MV, et al: Effect of a short course of
34. Mantel N: Evaluation of survival data and two new rank order
neoadjuvant hormonal therapy on the response to subsequent androgen
statistics arising in its consideration. Cancer Chemother Rep 5:163-170, 1966
suppression in prostate cancer patients with relapse after radiotherapy: A
35. Gray RL: A class of K-sample tests for comparing the cumulative
secondary analysis of the randomized protocol RTOG 86-10. Int J Radiat
incidence of a competing risk. Ann Stat 16:1141-1154, 1988
36. Cox DR: Regression models and life tables. J R Stat Soc Series B
45. Brinker DA, Ross JS, Tran T-A, et al: Can ploidy of prostate
carcinoma diagnosed on needle biopsy predict radical prostatectomy stage
37. Pollack A, Zagars GK: Pre-treatment prognostic factors for prostate
cancer patients treated with external beam radiotherapy, in Greco C, Zelefsky
46. Ahlgren G, Falmer U, Gadaleanu V, et al: Evaluation of DNA ploidy
MJ (eds.): Radiotherapy of Prostate Cancer, Harwood Academic, Singapore,
combined with a proliferation index of imprints from core needle biopsies in
prostate cancer. Eur Urol 36:314-319, 1999
Information downloaded from jco.ascopubs.org and provided by UNIVERSITAETS UND LANDESBIBLIO on May 9, 2008
Copyright 2003 by the American Society of Clinical Oncology. All rights reserved.
D I A R I O O F I C I A L 4 6 6 1 1 D E 2 0 0 7 MINISTERIO DE LA PROTECCIÓN SOCIAL RESOLUCION NÚMERO 0676 (marzo 9 de 2007) Por la cual se establece el reglamento técnico de emergencia a través del cual se adopta el Plan Nacional de Control de Residuos de Medicamentos Veterinarios y otras Sustancias Químicas 2007 que deben cumplir los productos acuícolas para consumo h
QR TRAVEL TRAIN QUEENSLAND LONG-DISTANCE TRAINS Reservations are necessary on all QR TravelTrain services QC1 BRISBANE - ROCKHAMPTON - TOWNSVILLE - CAIRNS NG. Quadruple track Brisbane-Northgate. Triple track Northgate-Lawnton. Double track Lawnton-Beerburrum, Callemondah-Rocklands, Nome-Townsville. Electrified Brisbane-Rockhampton. Track runs along streets briefly in North Bundaberg and i
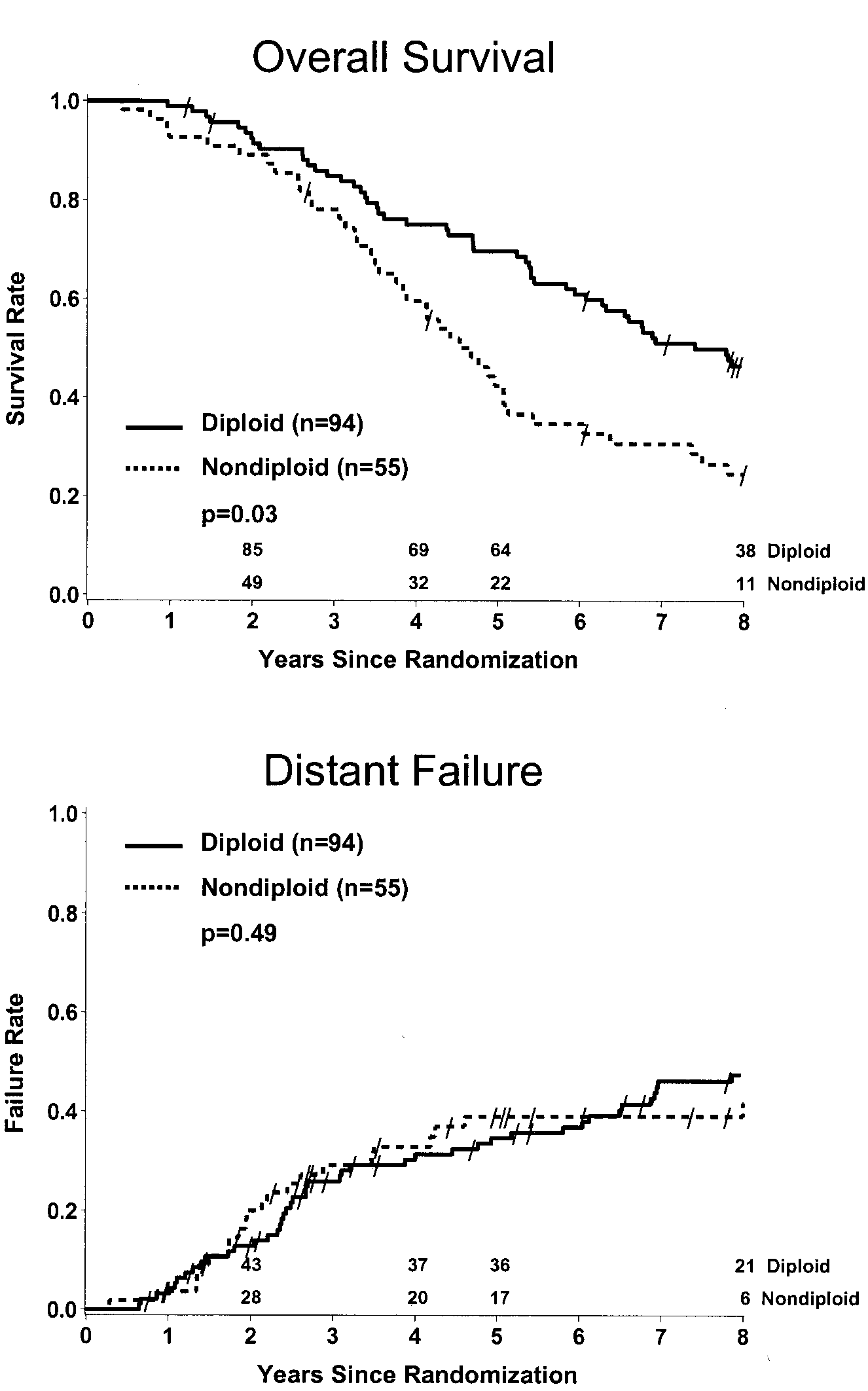 Fig 1. Kaplan-Meier survival analysis of overall sur-
Fig 1. Kaplan-Meier survival analysis of overall sur-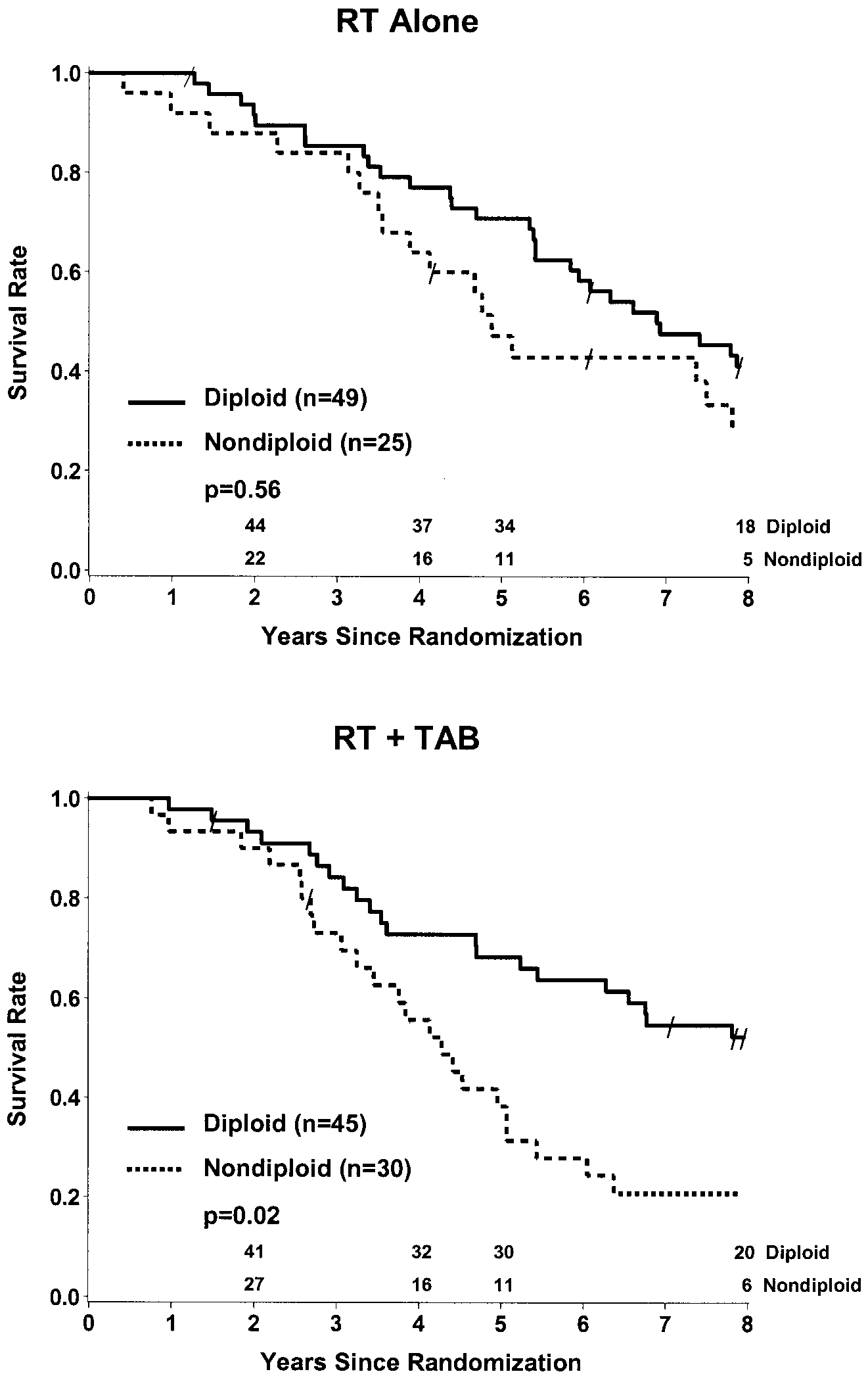 DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 2. Kaplan-Meier analysis of overall survival for
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 2. Kaplan-Meier analysis of overall survival for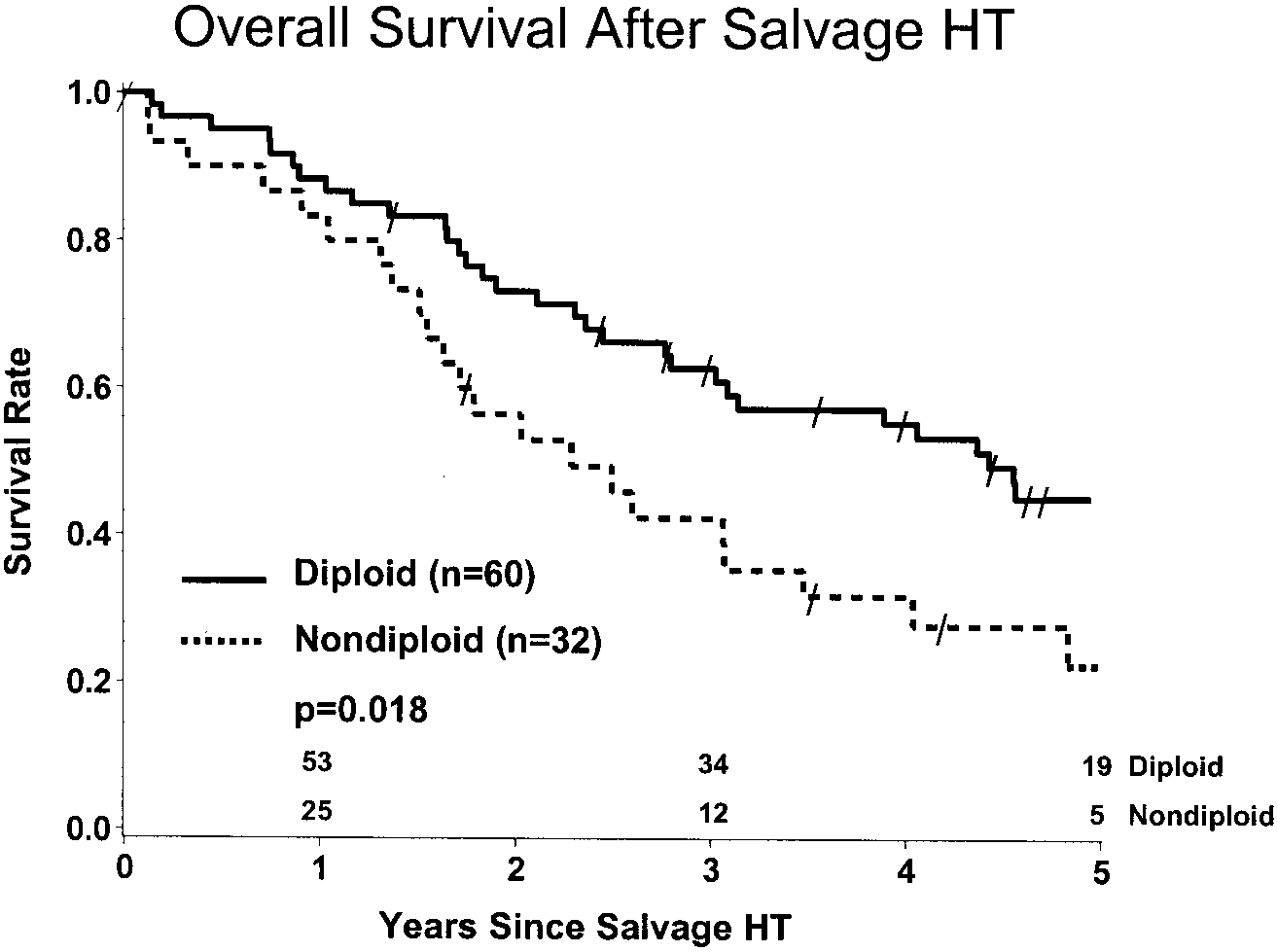 DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Table 6. Adjusted Cox Proportional Hazards Regression Analyses (n ؍ 429)
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Table 6. Adjusted Cox Proportional Hazards Regression Analyses (n ؍ 429)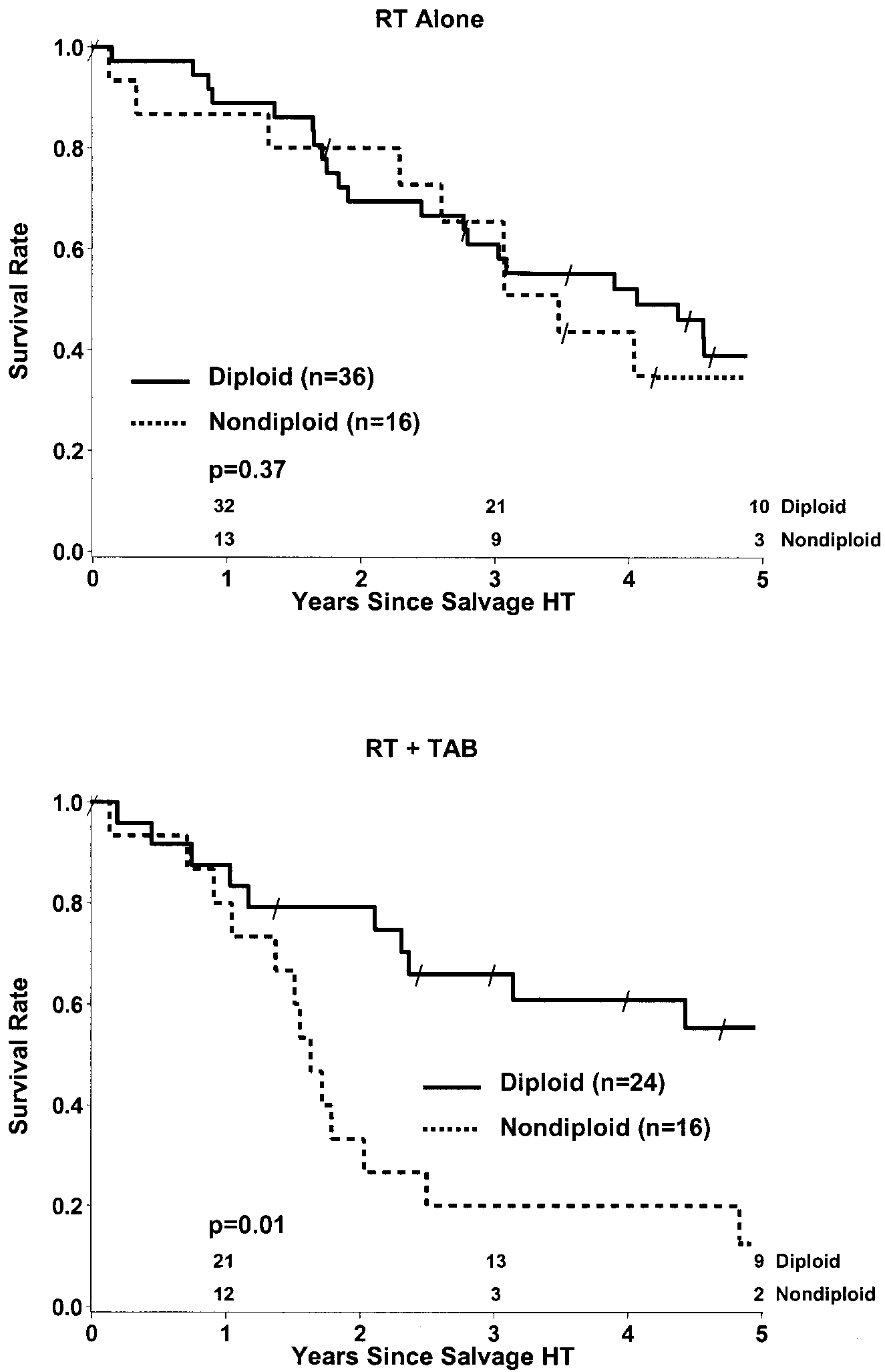 Fig 4. Kaplan-Meier analysis of overall survival after
Fig 4. Kaplan-Meier analysis of overall survival after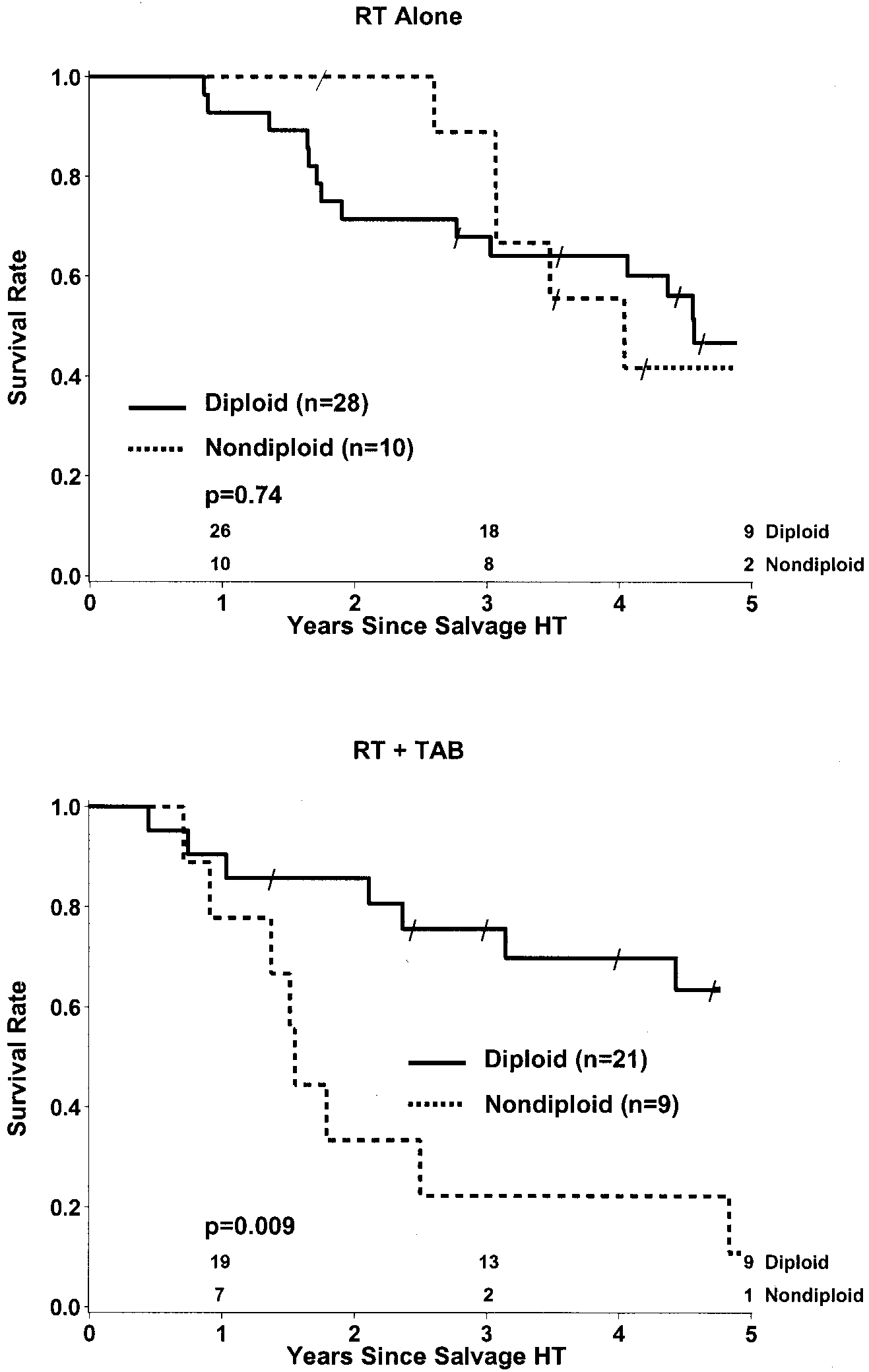 DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 5. Kaplan-Meier analysis of overall survival after
DNA NONDIPLOIDY AND SALVAGE HORMONE THERAPY
Fig 5. Kaplan-Meier analysis of overall survival after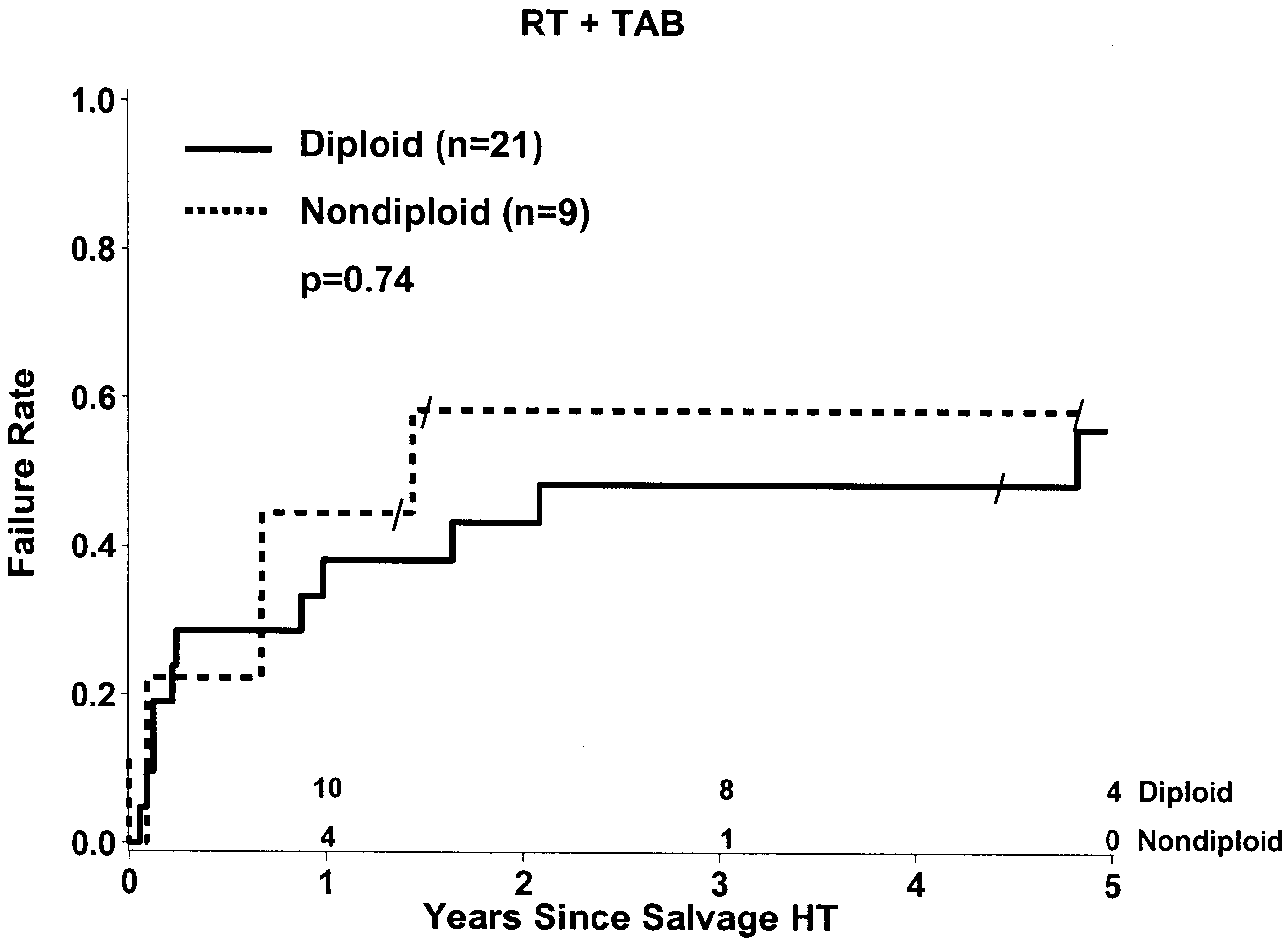 Fig 6. Kaplan-Meier analysis of the relationship of
Fig 6. Kaplan-Meier analysis of the relationship of