L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Phoslock.com.br
Veerle P. Persy, Geert J. Behets, An R. Bervoets, Marc E. De Broe, and Patrick C. D'HaeseUniversity of Antwerp, Antwerp, Belgium
ABSTRACT
Accumulation of inorganic phosphate due to renal functional
and its effects in bone, liver and brain are discussed. Although
impairment contributes to the increased cardiovascular mortal-
lanthanum is a metal cation its effects are not comparable to
ity observed in dialysis patients. Phosphate plays a causative
those of aluminum. Indeed, in clinical studies no toxic effects
role in the development of vascular calcification in renal fail-
of lanthanum have been reported after up to four years of fol-
ure; treatment with calcium-based phosphate binders and vita-
low-up. The bioavailability of lanthanum is extremely low. The
min D can further increase the Ca × PO product and add to the
effects observed in bone are due to phosphate depletion, with
risk of ectopic mineralization. The new generation of calcium-
no signs of direct bone toxicity yet observed in rats or humans.
free phosphate binders, sevelamer and lanthanum, can control
The liver is the main route of excretion for lanthanum carbon-
hyperphosphatemia without adding to the patients calcium
ate, which can be localized in the lysosomes of hepatocytes. No
load. In this article, the metabolism of lanthanum carbonate
lanthanum could be detected in brain tissue.
Inorganic phosphate plays a role in important cellular
The disturbed mineral metabolism that accompanies
functions such as energy storage and signaling, and in
chronic renal failure contributes to the development of
bone mineralization. Loss of renal function limits phos-
ectopic calcification. Vascular calcification is a promi-
phate excretory capacity and causes an increase in serum
nent feature of cardiovascular disease in uremic patients.
phosphate level, which together with low ionized cal-
In a landmark article, Goodman et al. (7) showed that
cium levels, contributes to the development of secondary
coronary artery calcification is already present in young
hyperparathyroidism and renal osteodystrophy (ROD).
hemodialysis patients, shows rapid progression, and is
In the long run, these factors cause parathyroid gland
associated with increased serum phosphate and calcium-
hyperplasia and autonomous parathyroid hormone (PTH)
phosphate product. Vascular calcification in dialysis
production (tertiary hyperparathyroidism) (1,2).
patients is associated with a higher daily calcium intake
Phosphate accumulation in the body and hyperphos-
from calcium-based phosphate binders (7-9). Hence
phatemia are associated with an increased mortality risk.
attempts to control serum PTH levels with calcium-
In hemodialysis patients, serum phosphate levels greater
based phosphate binders and vitamin D supplements can
than 6.5 mg /dl, as well as elevated calcium-phosphate
further increase the calcium-phosphate product and the
product (greater than 72 mg2/dl2) are associated with a
risk for ectopic calcification and its associated cardio-
significantly increased mortality risk (3). In patients with
vascular mortality. In addition to increased calcification
chronic kidney disease (CKD), there is a linear increase
of atherosclerotic plaques in the vessel (neo)intima,
in mortality as serum phosphate rises above 3.5 mg /dl, a
patients on dialysis also show characteristic calcifica-
level that is still in the normal range (4). Phosphate reten-
tions of the vascular media (arteriosclerosis or Möncke-
tion mainly increases cardiovascular mortality, such as
berg sclerosis), which were recently shown to also
death through coronary artery disease and sudden death
contribute significantly to the excess cardiovascular mor-
(5). Physiologic phosphate homeostasis is controlled by
tality observed in uremic patients (8).
a number of phosphaturic factors in addition to PTH,
In vitro studies have elegantly demonstrated that ele-
such as FGF-23 and the so-called phosphatonins, while
vated phosphate and calcium levels are causative players
no phosphate retention-inducing factors have been iden-
in the cell-mediated process of uremia-related calcifica-
tified so far. Overall, studies indicate that accumulation
tion of the vascular tunica media (10). In cultured human
of phosphate and concomitant hyperphosphatemia form
aortic smooth muscle cells, a dose-dependent increase in
a serious threat to survival in CKD (6).
mineral deposition was observed, together with loss ofsmooth muscle cell differentiation markers and conver-sion of smooth muscle cells to an osteogenic phenotype,
Address correspondence to : Veerle P. Persy, MD, PhD,
characterized by expression of the osteoblast transcrip-
University of Antwerp, Universiteitsplein 1, B-2610 Wilrijk,
tion factor cbfa-1 and the osteoblast protein osteocalcin
Antwerp, Belgium, or e-mail: veerle.persy@ua.ac.be.
(11,12). These effects could be inhibited by blocking
Seminars in Dialysis-Vol 19, No 3 (May-June) 2006
phosphate entrance into the cell through the sodium/
phosphorus cotransporter Pit-1 with phosphonoformic
Fig. 1. Metabolism of two trivalent cations: aluminum and lanthanum. In contrast to aluminum, there is no increased deposition of lanthanum in
end-stage renal disease compared to patients with normal renal function. Adapted from Behets et al. (23).
acid (11). In epigastric arteries of uremic patients under-
biological ligands are the carboxyl and phosphate groups
going transplantation, the presence of calcification was
( PO3−) with which it can form very tight complexes.
associated with expression of cbfa-1 (13), alkaline phos-
In comparison with aluminum, lanthanum accumu-
phatase, and the bone matrix proteins osteopontin, bone
lates to a lesser extent in the body of dialysis patients,
sialoprotein, and collagen type I (14), confirming the
mainly because of its ultralow gastrointestinal absorp-
cell biological parallels between vascular calcification
tion and biliary elimination of the small absorbed
and bone formation. Several proteins possessing a high
fraction (Fig. 1). Studies have shown that the absolute
calcium affinity, such as matrix Gla protein, osteoprote-
bioavailability of lanthanum in man is less than 0.002%,
grin, osteopontin, and fetuin, may modulate the ectopic
with the majority of an oral dose being excreted in the
calcification process in the vasculature by their ability to
feces. Biliary elimination (80%) and direct transport
act as natural inhibitors of these calcifications.
across the gut wall into the lumen (13%) represent the
The available calcium-free phosphate binders include
main routes of elimination. Therefore the elimination
sevelamer hydrochloride (a nonaluminum, noncalcium-
of lanthanum is not dependent on renal function; of a
containing hydrogel of cross-linked poly(allylamine
lanthanum dose of 1 g/day in healthy volunteers, only
hydrochloride) that binds phosphate anions through
0.00003% was excreted in the urine (19), indicating that,
ionic exchange with chloride) and more recently, lantha-
compared with individuals with normal renal function,
num carbonate. These products can control phosphate
chronic renal insufficiency patients are not at an
levels without inducing calcium overload. In comparison
increased risk for accumulation of the element. This has
with calcium-based phosphate binder therapy, treatment
been confirmed in several phase 1 clinical studies, which
with sevelamer slowed down the progression of coronary
have indicated similar plasma exposure and pharmaco-
artery and aortic calcification in dialysis patients (15,16).
kinetics of lanthanum in dialysis patients and healthy
However, apart from its phosphate binding activity, seve-
lamer also acts as a bile acid sequestrant (17), resulting
This is in contrast to orally administered aluminum, of
in lowering of total and low-density lipoprotein (LDL)
which 0.01- 0.10% is absorbed from the gastrointestinal
cholesterol, and can induce acidosis by exchange of
tract (Fig. 1) (20,21), and which is mainly eliminated via
bicarbonate with chloride ions (18). These additional
the kidney, biliary excretion being negligible. When
effects can also influence the calcification process. How-
calcium citrate was coadministered with aluminum hydro-
ever, no studies on the effect of lanthanum carbonate,
xide (2.4 g/day), aluminum excretion increased from 70 -
which is a pure phosphate binder, on vascular calcifica-
120 mg/day up to 350 - 603 mg/day (21). Citrate does not
tion in dialysis patients are available yet.
influence gastrointestinal absorption of lanthanum.
Lanthanum belongs to the group of elements known as
the "lanthanides." It is the most electropositive (cationic)element of the rare earth group, is uniformly trivalent,
and its binding is almost exclusively ionic. It is ahard "acceptor" with an overwhelming preference for
In experimental studies, no effects of lanthanum on
oxygen-containing anions. Therefore the most common
bone have been observed in animals with normal renal
bone calcium, knowledge of the molar bone cation:calcium ratio is of particular interest for a better under-standing of its potential to disrupt bone mineral struc-ture. Regarding lanthanum (molecular weight 139), thehighest concentration observed in the bone of dialysispatients was 9.5 µg/g (67 nmol/g) wet weight after 4.5years of treatment with lanthanum carbonate (2.5 -3.0 g /day). Considering a bone calcium concentration of 120mg /g (3 mmol/g) and assuming a homogeneous distribu-tion of lanthanum throughout the bone, the molar bonelanthanum:calcium ratio would be as low as 2 × 10−5,that is, only 1 out of 50,000 calcium atoms would bereplaced by lanthanum. If one assumes lanthanum toaccumulate in only 1% of the total bone volume, stillonly 1 out of 500 calcium ions would be replaced bylanthanum, and any effect on either bone mineral crystalnucleation, crystal growth, or structure would not readilybe expected. Applying the same reasoning to aluminumand assuming the total amount of the element (up to50 µg/g, 1.8 µmol/g) is localized in only 1% of the total
Fig. 2. Using the highly sensitive methodology of X-ray fluore-
bone volume (a reasonable assumption in patients with
scence, lanthanum was found at several sites in human bone.
aluminum-related osteomalacia in which the element islocalized at the osteoid-calcification front of the bone),
function loaded with lanthanum at doses up to 2000 mg /
the molar bone aluminum:calcium ratio would be
kg /day for 2 years (22). On the other hand, rats with
6 × 10−2. In other words, 1 out of 16 calcium atoms
chronic renal failure loaded with doses of 1000 -2000
would be replaced by aluminum, increasing the probabil-
mg/kg/day for 12 weeks showed an impairment of bone
ity of toxic effects at the level of apatite nucleation, crys-
mineralization (23). However, several further studies
produced evidence that the observed lesions were phar-
A randomized, comparator-controlled, parallel-group,
macologically mediated and resulted from phosphate
open-label study was set up to assess the evolution of
depletion induced by the administration of high doses of
ROD in dialysis patients receiving treatment with lantha-
lanthanum carbonate rather than being the consequence
num carbonate versus calcium carbonate for 1 year, with
of a direct toxic effect of the compound.
particular emphasis on the possible development of
Further evidence of the absence of any direct toxicity
aluminum-like bone diseases, that is, osteomalacia or
of lanthanum on bone includes the fact that bone lantha-
num concentration does not correlate with the various
Paired bone biopsy specimens were taken in 63
histomorphometric bone parameters, and the effects of
patients at the start and after 12 months of treatment with
lanthanum on bone mimic those induced by feeding a low-
either lanthanum carbonate (n = 33) or calcium carbon-
phosphate diet, are normalized with phosphate repletion
ate (n = 30). The bone biopsies were assessed for lan-
(24), and are similar to those observed in rats treated
thanum content, and were examined for histologic and
with sevelamer (25). Moreover, whereas in dialysis
patients with aluminum-related bone disease (expressed
After 1 year of lanthanum carbonate treatment, serum
either as osteomalacia or adynamic bone) aluminum
lanthanum levels were slightly increased, although not
accumulation was accompanied by a decreased number/
dose-dependently (mean serum levels ranging from 0.51
activity of osteoblasts (26), such an effect was not seen
to 1.08 ng /ml), and reached a plateau within 12 weeks of
after lanthanum loading in either rats or humans (27).
treatment. After 1 year of treatment with lanthanum car-bonate, bone lanthanum levels did not exceed 5.5 µg/gwet weight (median 1.8 µg/g).
The distribution of the different types of ROD at base-
Studies in animals and humans have shown that lan-
line was comparable between the two groups, with
thanum is deposited in bone and liver. Localization of
mixed ROD being the most common type. After 1 year of
lanthanum in bone, obtained by means of X-ray fluorescence
treatment, lanthanum carbonate was associated with a
at the European Synchrotron Radiation Facility, Greno-
reduction in each of the more extreme forms of ROD
ble, France, showed the element to be present at both
(i.e., hyperparathyroidism, adynamic bone disease, and
active and quiescent sites of bone mineralization, inde-
osteomalacia). Calcium carbonate was associated with
pendent of the type of ROD, as well as diffusely distrib-
an increase in the proportion of patients with hyper-
uted throughout the mineralized bone matrix, especially
parathyroidism or adynamic bone disease. Overall, five
in rats and humans with increased bone turnover (Fig. 2).
out of seven (71%) lanthanum carbonate-treated patients
Lanthanum was also found in cells in close proximity to
with low-turnover bone disease (adynamic bone or
the resorption lacunae (osteoclasts, macrophages) (28).
osteomalacia) at baseline, and 80% (four out of five) of
As the accumulation of cations in bone goes along
those with baseline hyperparathyroidism evolved toward
with an interaction between the cation of interest and
a normalization in bone turnover, compared with three
Fig. 4. Lanthanum in a crystalline, granular-like form was found in
the lysosomes (black arrows) of the hepatocytes. No lanthanum was
Fig. 3. Liver enzymes after treatment with lanthanum carbonate or
detected in other organelles such as mitochondria, nucleus, cytoplasm, or
Golgi apparatus. Transmission electron microscopy of the liver tissueof lanthanum loaded rats. Rats were loaded with a very high dose of0.3 mg / kg /day intravenously over 4 weeks (31).
out of seven (42%) and three out of six (50%) calciumcarbonate-treated patients, respectively.
In summary, the proportion of patients with adynamic
bone disease, osteomalacia, or hyperparathyroidism in
For the energy dispersive X-ray (EDX) analytical
the lanthanum carbonate group decreased from 36% to
work, an atmospheric thin window Oxford instrument
18% after 1 year of treatment, whereas the number of
was connected to a CM20 TEM instrument equipped
patients with these types of ROD increased from 43% to
with a lanthanum hexaboride (LaB ) single crystal fila-
53% in the calcium carbonate group. In the lanthanum
ment operating at 200 kV, 120 kV, or 80 kV. For the elec-
group, no aluminum-like effects on bone were observed.
tron energy loss spectroscopy (EELS), a postcolumnGIF2000 instrument was used in connection with anUltratwin CM30 TEM instrument equipped with a field
emission gun (FEG) and operating at 300 kV. The com-bined use of these techniques indicated lanthanum to be
Since the liver is the main excretory organ of lantha-
present in the lysosomes of the hepatocytes (Fig. 4). No
num, it is not surprising to find some deposition of the
lanthanum was detected in mitochondria, the nucleus, or
element at this site. However, clinical studies with up to
cytoplasm. Furthermore, most of the lanthanum was
4 years of follow-up have not disclosed any hepatotoxic
found in lysosomes at the biliary pole of the hepatocyte
effect of the drug in patients treated with this phosphate
and within the bile canaliculus (30).
binder (Fig. 3). Twelve weeks of lanthanum loading byoral gavage of 2000 mg/kg/day to rats with moderaterenal failure resulted in concentrations of 1.5 µg/g and
3.5 µg/g of lanthanum in bone and liver, respectively. Brain levels remained below the detection limit. Other
In a number of experimental studies, lanthanum was
tissues such as heart, skin, and lung showed no tissue
determined to be in several regions of the brain after
administration of intravenous doses of 30-300 mg/kg/
In order to identify the localization of lanthanum in
day over 4 weeks and oral gavage of 1500 mg/kg/day. No
the liver, lanthanum chloride was administered by daily
lanthanum could be detected (less than 6 ng/g).
intravenous injection to rats with normal renal functionat a 0.3 mg/kg dose over 4 weeks. The total liver lantha-num concentrations varied between 30 and 50 µg/g.
Liver fragments of treated as well as untreated animals
were fixed in 4% formaldehyde in phosphate buffer and
Lanthanum carbonate is an effective aluminum- and
postfixed in reduced osmium tetroxide (OsO ). After
calcium-free phosphate binder. The drug is well tolerated
dehydration and embedding in Epon, 100 nm, 500 nm,
and the reported incidence of gastrointestinal side effects
and 1000 nm sections were prepared. These were exam-
is comparable with reports on calcium-containing phos-
ined by conventional imaging in a Zeiss transmission
electron microscope (TEM) at 50 kV or a Philips TEM
Available bone biopsy data in dialysis patients treated
(at 80 kV) either without or after counterstaining with
for up to 4 years with lanthanum carbonate indicate low-
lead citrate, at magnifications varying between 1800×
level bone deposition, the highest concentration ever
measured in any patient being 9.4 µg/g. Ultrastructural
localization indicates a heterogeneous distribution of
12. Giachelli CM: Ectopic calcification: new concepts in cellular regulation. Z
lanthanum in the bone of rats and man. The low molar
13. Moe SM, Duan D, Doehle BP, O'Neill KD, Chen NX: Uremia induces the
lanthanum:calcium ratio is unlikely to cause physico-
osteoblast differentiation factor Cbfa1 in human blood vessels. Kidney Int
chemical interactions of the metal with hydroxyapatite
14. Moe SM, O'Neill KD, Duan D, Ahmed S, Chen NX, Leapman SB, Fineberg
development and structure. Furthermore, no adverse cell
N, Kopecky K: Medial artery calcification in ESRD patients is associated
biological effects of lanthanum on osteoblasts have been
with deposition of bone matrix proteins. Kidney Int 61:638 - 647, 2002
15. Chertow GM, Burke SK, Raggi P: Sevelamer attenuates the progression of
coronary and aortic calcification in hemodialysis patients. Kidney Int
The presence of lanthanum in the bile and in the lyso-
somes of the liver is consistent with excretion of lanthanum
16. Block GA, Spiegel DM, Ehrlich J, Mehta R, Lindbergh J, Dreisbach A,
by the liver via the transferrin receptor-endosomal-
Raggi P: Effects of sevelamer and calcium on coronary artery calcification inpatients new to hemodialysis. Kidney Int 68:1815 -1824, 2005
lysosomal-bile canaliculus pathway. Clinical studies of
17. Braunlin W, Zhorov E, Guo A, Apruzzese W, Xu Q, Hook P, Smisek DL,
up to 4 years have not disclosed any hepatotoxic effect of
Mandeville WH, Holmes-Farley SR: Bile acid binding to sevelamer HCl. Kidney Int 62:611- 619, 2002
the drug in patients treated with this phosphate binder. In
18. Brezina B, Qunibi WY, Nolan CR: Acid loading during treatment with seve-
summary, these data indicate that the heavily protein
lamer hydrochloride: mechanisms and clinical implications. Kidney Int Suppl
bound lanthanum follows a transcellular pathway during
19. Damment SJP, Gill M: The pharmacokinetics and tissue distribution of lan-
thanum carbonate (Fosrenol), a new non-aluminum, non-calcium phosphate
No lanthanum could be detected in the brain of rats
binder [abstract]. J Am Soc Nephrol 14:204A, 2003
fed orally or after intravenous administration of high
20. Jouhanneau P, Raisbeck GM, Yiou F, Lacour B, Banide H, Drueke TB: Gas-
trointestinal absorption, tissue retention, and urinary excretion of dietary alu-
doses of lanthanum over 4 weeks. Further studies unrave-
minum in rats determined by using 26Al. Clin Chem 43:1023-1028, 1997
ling the speciation of lanthanum in biological fluids will
21. Coburn JW, Mischel MG, Goodman WG, Salusky IB: Calcium citrate mark-
edly enhances aluminum absorption from aluminum hydroxide. Am J Kidney
contribute to a further understanding of its metabolism
22. Damment SJP, Greaves P, Downes N: The toxicology of lanthanum carbon-
ate (Fosrenol), a new non-aluminum, non-calcium phosphate binder[abstract]. J Am Soc Nephrol 14:204A, 2003
23. Behets GJ, Dams G, Vercauteren SR, Damment SJ, Bouillon R, De Broe ME,
D'Haese PC: Does the phosphate binder lanthanum carbonate affect bone inrats with chronic renal failure? J Am Soc Nephrol 15:2219 -2228, 2004
24. Damment SJ, Shen V: Assessment of effects of lanthanum carbonate with
1. Silver J, Kilav R, Naveh-Many T: Mechanisms of secondary hyperparathy-
and without phosphate supplementation on bone mineralization in uremic
roidism. Am J Physiol Ren Physiol 283:F367-F376, 2002
rats. Clin Nephrol 63:127-137, 2005
2. Silver J: Pathogenesis of parathyroid dysfunction in end-stage renal disease.
25. Behets GJ, Gritters M, Dams G, De Broe ME, D'Haese PC: Effects of effi-
Adv Ren Replace Ther 9:159-167, 2002
cient phosphate binding on bone in chronic renal failure rats. Ren Fail
3. Block GA, Hulbert-Shearon TE, Levin NW, Port FK: Association of serum
phosphorus and calcium × phosphate product with mortality risk in chronic
26. Rodriguez M, Felsenfeld AJ, Llach F: Aluminum administration in the rat
hemodialysis patients: a national study. Am J Kidney Dis 31:607- 617, 1998
separately affects the osteoblast and bone mineralization. J Bone Miner Res
4. Kestenbaum B, Sampson JN, Rudser KD, Patterson DJ, Seliger SL, Young B,
Sherrard DJ, Andress DL: Serum phosphate levels and mortality risk among
27. Behets GJ, Bervoets AJ, Dams G, Damment SJ, De Broe ME, D'Haese PC:
people with chronic kidney disease. J Am Soc Nephrol 16:520 -528, 2005
Effects of lanthanum and strontium on osteoblasts in chronic renal failure
5. Ganesh SK, Stack AG, Levin NW, Hulbert-Shearon T, Port FK: Association
rats [abstract]. J Am Soc Nephrol 14:898A, 2003
of elevated serum PO(4), Ca × PO(4) product, and parathyroid hormone with
28. Behets GJ, Verberckmoes SC, Oste L, Bervoets AR, Salome M, Cox AG,
cardiac mortality risk in chronic hemodialysis patients. J Am Soc Nephrol
Denton J, De Broe ME, D'Haese PC: Localization of lanthanum in bone of
chronic renal failure rats after oral dosing with lanthanum carbonate. Kidney
6. Prie D, Beck L, Urena P, Friedlander G: Recent findings in phosphate
homeostasis. Curr Opin Nephrol Hypertens 14:318-324, 2005
29. D'Haese PC, Spasovski GB, Sikole A, Hutchison A, Freemont TJ, Sulkova
7. Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y,
S, Swanepoel C, Pejanovic S, Djukanovic L, Balducci A, Coen G, Sulowicz
Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB: Coronary-artery
W, Ferreira A, Torres A, Curic S, Popovic M, Dimkovic N, De Broe ME: A
calcification in young adults with end-stage renal disease who are undergo-
multicenter study on the effects of lanthanum carbonate (Fosrenol) and cal-
ing dialysis. N Engl J Med 342:1478 -1483, 2000
cium carbonate on renal bone disease in dialysis patients. Kidney Int Suppl
8. London GM, Guerin AP, Marchais SJ, Metivier F, Pannier B, Adda H:
Arterial media calcification in end-stage renal disease: impact on all-cause
30. Yang Z, Schryvers D, Roels F, D'Haese PC, De Broe ME: Demonstration of
and cardiovascular mortality. Nephrol Dial Transplant 18:1731-1740, 2003
La in liver cells by EDX, EELS and HRTEM. J Microsc submitted
9. Chertow GM, Raggi P, Chasan-Taber S, Bommer J, Holzer H, Burke SK:
31. D'Haese PC, Yang Z, Schryvers D, Roels F, Behets GJ, Verberckmoes SC,
Determinants of progressive vascular calcification in haemodialysis patients.
Bervoets AJ, Dauwe S, Salome M, De Broe ME: Lanthanum is localized
Nephrol Dial Transplant 19:1489-1496, 2004
(sub)cellularly in lysosomes of the liver [abstract]. J Am Soc Nephrol
10. Giachelli CM: Vascular calcification. in vitro evidence for the role of inor-
ganic phosphate. J Am Soc Nephrol 14:S300 -S304, 2003
32. Hutchison A: Analysis of liver function and hepatobiliary adverse event data
11. Jono S, McKee MD, Murry CE, Shioi A, Nishizawa Y, Mori K, Morii H,
from 2000 dialysis patients participating in clinical trials on the new phos-
Giachelli CM: Phosphate regulation of vascular smooth muscle cell calcifica-
phate binder, lanthanum carbonate [abstract]. Nephrol Dial Transplant
tion. Circ Res 87:E10 -E17, 2000
LINCOLN SURGERY ENDOSCOPY SERVICES Patient Name:_________________________________________ Your Family Doctor is:___________________________ Reason for today's exam: Height: ________ Weight: _________ Please list all medications, including over-the-counter and herbal remedies below. Medicine Why Taking Medicine Why Taking **List all ALLERGIES including type of allergy
Unsere Leistungsangebote Diagnostik und Therapie der Erkrankungen Dr. Rudolf Krause Kluckstr. 38 10785 Berlin Tel.: 030-2629296 - Einsatz bei Hauterkrankungen Der gezielte, Resistogramm - gestützte Einsatz wirk-samer Antibiotika bei unseren Wohnungstieren ist auch bei Hauterkrankungen unausweichlich gewor-den. In aller Regel haben Hauterkran
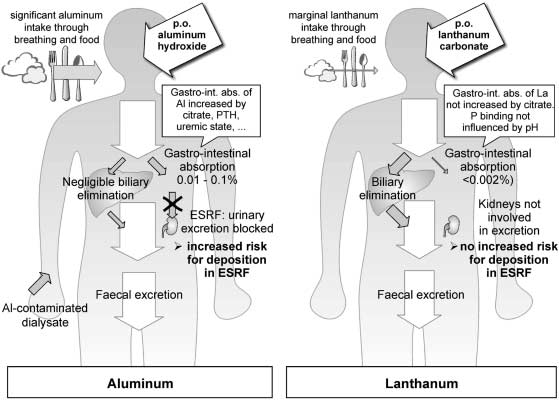 Fig. 1. Metabolism of two trivalent cations: aluminum and lanthanum. In contrast to aluminum, there is no increased deposition of lanthanum in
end-stage renal disease compared to patients with normal renal function. Adapted from Behets et al. (23).
Fig. 1. Metabolism of two trivalent cations: aluminum and lanthanum. In contrast to aluminum, there is no increased deposition of lanthanum in
end-stage renal disease compared to patients with normal renal function. Adapted from Behets et al. (23).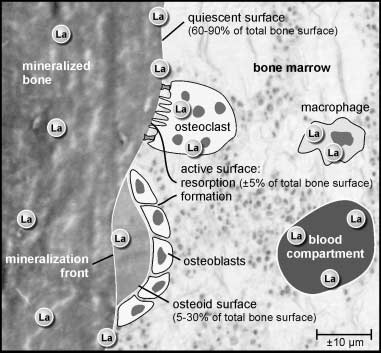 bone calcium, knowledge of the molar bone cation:calcium ratio is of particular interest for a better under-standing of its potential to disrupt bone mineral struc-ture. Regarding lanthanum (molecular weight 139), thehighest concentration observed in the bone of dialysispatients was 9.5 µg/g (67 nmol/g) wet weight after 4.5years of treatment with lanthanum carbonate (2.5 -3.0 g /day). Considering a bone calcium concentration of 120mg /g (3 mmol/g) and assuming a homogeneous distribu-tion of lanthanum throughout the bone, the molar bonelanthanum:calcium ratio would be as low as 2 × 10−5,that is, only 1 out of 50,000 calcium atoms would bereplaced by lanthanum. If one assumes lanthanum toaccumulate in only 1% of the total bone volume, stillonly 1 out of 500 calcium ions would be replaced bylanthanum, and any effect on either bone mineral crystalnucleation, crystal growth, or structure would not readilybe expected. Applying the same reasoning to aluminumand assuming the total amount of the element (up to50 µg/g, 1.8 µmol/g) is localized in only 1% of the total
Fig. 2. Using the highly sensitive methodology of X-ray fluore-
bone volume (a reasonable assumption in patients with
scence, lanthanum was found at several sites in human bone.
bone calcium, knowledge of the molar bone cation:calcium ratio is of particular interest for a better under-standing of its potential to disrupt bone mineral struc-ture. Regarding lanthanum (molecular weight 139), thehighest concentration observed in the bone of dialysispatients was 9.5 µg/g (67 nmol/g) wet weight after 4.5years of treatment with lanthanum carbonate (2.5 -3.0 g /day). Considering a bone calcium concentration of 120mg /g (3 mmol/g) and assuming a homogeneous distribu-tion of lanthanum throughout the bone, the molar bonelanthanum:calcium ratio would be as low as 2 × 10−5,that is, only 1 out of 50,000 calcium atoms would bereplaced by lanthanum. If one assumes lanthanum toaccumulate in only 1% of the total bone volume, stillonly 1 out of 500 calcium ions would be replaced bylanthanum, and any effect on either bone mineral crystalnucleation, crystal growth, or structure would not readilybe expected. Applying the same reasoning to aluminumand assuming the total amount of the element (up to50 µg/g, 1.8 µmol/g) is localized in only 1% of the total
Fig. 2. Using the highly sensitive methodology of X-ray fluore-
bone volume (a reasonable assumption in patients with
scence, lanthanum was found at several sites in human bone.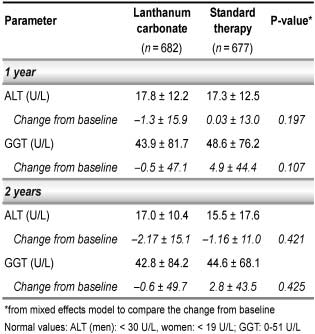
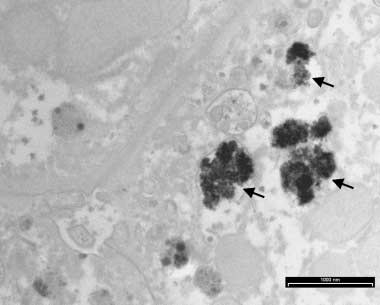 Fig. 4. Lanthanum in a crystalline, granular-like form was found in
the lysosomes (black arrows) of the hepatocytes. No lanthanum was
Fig. 3. Liver enzymes after treatment with lanthanum carbonate or
detected in other organelles such as mitochondria, nucleus, cytoplasm, or
Golgi apparatus. Transmission electron microscopy of the liver tissueof lanthanum loaded rats. Rats were loaded with a very high dose of0.3 mg / kg /day intravenously over 4 weeks (31).
Fig. 4. Lanthanum in a crystalline, granular-like form was found in
the lysosomes (black arrows) of the hepatocytes. No lanthanum was
Fig. 3. Liver enzymes after treatment with lanthanum carbonate or
detected in other organelles such as mitochondria, nucleus, cytoplasm, or
Golgi apparatus. Transmission electron microscopy of the liver tissueof lanthanum loaded rats. Rats were loaded with a very high dose of0.3 mg / kg /day intravenously over 4 weeks (31).