L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Michiganear.com
and staff of the Michigan Ear Institute,
web site at www.michiganear.com Michigan Ear Institute higan Ear Institute (248) 865-4444 phone Jack M. Kartush, MD
ORS Dennis I. Bojrab, MD Michael J. LaRouere, MD John J. Zappia, MD, FACS Eric W. Sargent, MD, FACS Seilesh C. Babu, MD Eleanor Y. Chan, MD Providence Medical Building Beaumont Medical Building Oakwood Medical Building Providence Medical Center 248-865-4444 phone IntRODuCtIOn
Dizziness is a non-specific term that can represent a host of different symptoms. While it generally refers to an abnormal sensation of motion, it can also mean imbalance, lightheadedness, blacking out, staggering, disorientation, weakness, just to name a few. Symptoms can range from mild brief spells to severe spinning lasting hours accompanied by nausea and vomiting. For clarity of discussion, the common types of dizziness are defined below. Dizziness A general term that refers to an abnormal sense of balance and equilibrium. Imbalance Inability to keep one's balance especially when on the feet, e.g. standing or walking. Lightheadedness A near pass-out or faint-like sensation, similar to the feeling if one breath-holds for a prolonged period. Vertigo The sensation that you or your surroundings are moving, spinning or whirling.
Maintenance of balance requires that multiple organ systems in the body execute perfect coordination. The brain is the central processing center that man-ages incoming balance information from the various sense organs and outgoing information directed to the muscles and skeleton.
Sensory input comes from three main areas: vision, inner ear, and touch (from the feet and joints). Vision is an important cue to the brain and allows us to determine if we are moving relative to our surround-ings.
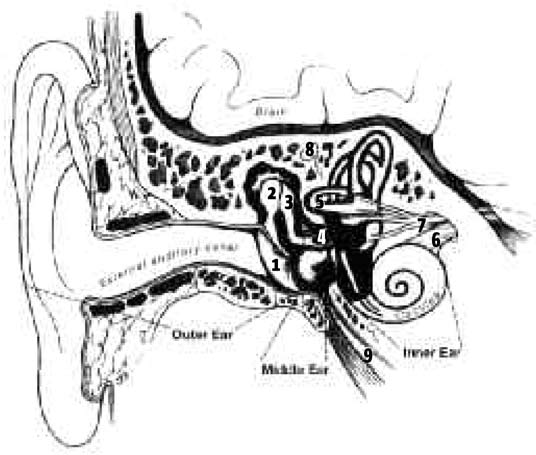
The inner ear serves two main functions: hearing and balance. There are two types of hearing: mechanical and nerve (or electric). The mechanical part of hear-ing begins with a sound wave arriving at the outer ear, which then travels down the ear canal to vibrate the ear drum and a chain of three tiny hearing bones in the middle ear. The inner ear resembles a snail. The coil portion is the cochlea, which is responsible for the sensory part of hearing. Like a telephone, it converts sound energy into an electrical signal which is relayed through the hearing (cochlear) nerve to the brain.
The other portion of the inner ear is the balance or vestibular system. There are three balance canals, each oriented in different angles. Rotational move-ment of the head causes a fluid shift within these
canals. This sends a signal to the brain via the ves-tibular nerve.
There are also two small compartments which contain sensory cells covered with small calcium crystals in a gelatin matrix. These compartments are responsible for sensing linear movement, such as swaying, rocking or bouncing. When the crystals of these compartments are dislodged, BPPV (benign paroxysmal positional vertigo) may result.
The inner ear fluids (perilymph and endolymph) undergo a natural recycling everyday. It is made from the brain's spinal fluid and is absorbed by the endolymphatic sac. In Meniere's syndrome, the sac fails to absorb enough fluid, leading to increased inner ear pressure that may cause dizziness and hearing loss.
The facial nerve is situated in close proximity to the ear. It moves the face and provides some of our taste sensation. Therefore, discussion of ear diseases and surgeries always emphasize preservation of the facial nerve due to its close anatomical relationship. MAIntEnAnCE OF BALAnCE
Balance is maintained by the coordinated interactions between the brain, inner ears, eyes, as well as various muscles and joints. A disturbance in any of these ar-eas may result in the subjective sensation of dizziness or unsteadiness. General medical ailments may also lead to dizziness due to interference with the brain and body's ability to integrate balance information.
The brain, reacting to abnormal or uncoordinated impulses, may respond such that the individual develops a false sense of movement (vertigo), result-ing in staggering or falling. The brain's influence on the body's glands and hormonal response may result in the commonly associated symptoms of nausea, vomiting or cold sweats.
Sensory input from the eyes as well as from the mus-cles and joints are sent to the brain, alerting us that the path we are following is bending to the right or that our head is tilted as we bend to pick up a dime. The brain interprets this information along with cues from the vestibular system and adjusts the muscles so that balance is maintained. Dizziness can occur when sensory information is distorted.
Some people feel dizzy at great heights, for instance, partly because they cannot focus on nearby objects to stabilize themselves. Without this frame of refer-ence, the individual may feel confusion, insecurity, and dizziness, which is sometimes resolved by sit-ting down. When on the ground, it is normal to sway slightly while standing.
Some scientists believe that motion sickness, a malady that affects sea, car and even space travelers, occurs when the brain receives conflicting sensory information about the body's motion and position. For example, when someone reads while riding in a car, the inner ear senses the movement of the ve-hicle, but the eyes gaze steadily on the book that is not moving. The resulting sensory conflict may lead to the typical symptoms of motion sickness: dizzi-ness, nausea, vomiting, and sweating.
Another form of dizziness occurs when we turn in a circle quickly several times and then stop suddenly. Turning moves the inner ear fluids. The inner ear indi-cates to the brain that rotation is occurring, yet other senses say we have stopped, therefore, we feel dizzy. CAuSES OF DIZZInESS
Dizziness can be grouped into types based on the malfunctioning portion(s) of the entire balance sys-tem. As mentioned, these include the inner ear, the brain, the eyes, and the limbs (neck, back, and leg muscles and joints which keep us upright). Inner Ear Dizziness Half of the inner ear is used for hearing (the cochlea) and the other half is used for balance (the labyrinth). If the labyrinth or vestibular nerve fail to func- tion, dizziness can result. Many types of maladies occur in the inner ear to cause dizziness, includ- ing Meniere's syndrome, labyrinthitis, positional vertigo, vestibular neuritis and tumors of the inner ear nerves. These usually cause imbalance, vertigo (spinning), and nausea. It can also be accompanied by tinnitus and hearing loss, if the nearby cochlea is affected. These diseases will be further explained later. Central Dizziness Central dizziness is caused by problems affecting the balance pathways of the brain. Symptoms usually include lightheadedness, disorientation, imbalance, and sometimes even blacking out. Causes of central dizziness include low blood sugar, low blood pres- sure, stroke, multiple sclerosis, migraine headaches, head injury, tumors, and the normal aging process, among others. Managing these types of dizziness involves identifying the underlying problem and treating the cause. Muscle-Joint Dizziness This type of dizziness is uncommon. If the muscles, joints or touch sensors of the limbs are not working well, it becomes difficult for the body to react to mo- tion, and makes it difficult to remain upright. Causes of muscle-joint dizziness include muscular dystro- phy, diabetic neuropathy, arthritis, joint replacement, and trauma. Imbalance and unsteadiness are com- mon in these situations. Visual Dizziness Uncoordinated eye muscles and poor vision can predispose to imbalance. The brain relies on critical
information from the eyes to coordinate balance. Motion sickness in the car or on a boat are examples of visual dizziness because the eyes are constantly adjusting to a moving visual field, which confuses the brain. This can lead to dizziness, nausea, and vomiting. Diagnosing the Cause of Dizziness Dizziness can be caused by various disturbances to one or more parts of the body. Based on history and physical findings, your physician may require further tests to complete a full evaluation. The necessary tests are determined at the time of examination, and may include hearing and balance tests, imaging (CT or MRI scans), bloodwork, etc. A general physical exam and neurological tests may also be required.
The most common test for dizziness is the electrony-stagmogram (ENG) or videonystagmogram (VNG). In this test, strength of the inner ears are evaluated, and coordination between eyes and brain checked. Prior to testing, it is important to avoid medications which can affect the results, such as valium, Antivert, alcohol, and others. When scheduling this test, make sure to cross check your list of medications.
Other tests include electrocochleography (ECoG) and vestibular evoked myogenic potentials (VEMP). These painless tests may be useful in determining the cause of dizziness in complex cases.
This detailed evaluation aims to rule out any serious or life threatening diseases, and to pinpoint the exact site of the problem. This lays the groundwork for ef-fective medical or surgical treatment.
Diagnosis can often be difficult. Frequently, multiple tests are conducted, and sometimes, tests may need to be repeated as a way of evaluating progress. Pa-tience and understanding are necessary on the part of the physician and patient alike. COMMOn tYPES OF DIZZInESS Benign Paroxysmal Positional Vertigo (BPPV) BPPV is the most common dizzy condition. In BPPV, vertigo is usually triggered by a change in head posi- tion, such as in rolling over in bed, tilting the head backward at the hairdresser's, or bending forward. BPPV is caused by tiny crystals that have dislodged into the balance canals which cause the sensation of spinning. The most common causes of BPPV are head trauma, viral infections of the inner ear, but often, it may start without any apparent cause.
Treatment of BPPV is usually an office repositioning maneuver that replaces the loosened crystals back into their original place within the inner ear. Once they heal back in place, dizziness resolves. Main-taining the head in the upright neutral position pro-motes healing. Following repositioning, certain head exercises can help reduce symptoms. Sometimes, repositioning may have to be repeated. Recurrence of BPPV despite successful repositioning occurs in 10-25% of patients. The OMNIAX is an omnidirec-tional chair designed specifically to aid repositioning in certain resistant cases of BPPV.
If the repositioning maneuver is ineffective, surgery may be required (see below - Posterior Canal Occlu-sion). Vestibular neuritis Neuritis (inflammation of a nerve) is often caused by a virus and may affect the balance (vestibular) nerve. When this occurs, the balance centers of the brain are overstimulated and results in intense dizziness and vertigo. Fortunately, vestibular neuritis usually subsides in time and does not typically recur. Certain medications can help in the initial phase to decrease the severity of symptoms, and later, balance therapy (vestibular rehabilitation) can speed recovery. Sur- gery is occasionally needed if symptoms persist. Meniere's Syndrome (Endolymphatic Hydrops) Meniere's Syndrome is a disorder of the inner ear caused by excess pressure in the endolymphatic flu- id compartment. The pressure is usually caused by excess inner ear sodium (salt). In addition to vertigo, which can last hours, patients may have fluctuat- ing hearing, tinnitus, and a feeling of fullness in the affected ear. Both ears may be affected. The cause of this disorder is not known. Excess salt intake, stress, weather changes, or allergies can trigger symptoms.
Treatment usually includes restriction of salt (so-dium) intake and use of a diuretic (water pill). Sometimes, anti-dizziness medications like Antivert or Valium can decrease the severity of the spells, but they do not cure the disease. Steroids can occasion- ally help, but because of side-effects, their use must be limited. If your doctor recommends water pills or steroids for you, please ask our nurses for the side effects information sheet to better inform you - and check with your family doctor.
In severe cases of Meniere's Disease, surgery or injection of the affected ear may be needed. Fortu-nately, there are many surgical options (discussed below). Of all these options, only Endolymphatic Sac Decompression aims to improve function of the inner ear. The remaining options selectively ablate (re- move or destroy) the malfunctioning balance nerve or labyrinth in the attempt to cure symptoms. Migraine Migraine is a common condition that can affect people of all ages and races. When it presents with headache, the diagnosis may be simple. However, many patients have symptoms related to migraine without the typical throbbing headaches. These symptoms are referred to as the "aura", and may include swaying or spinning sensations, visual dis- tortions, marked fatigue, motion intolerance, head
pressure or ear fullness. Hearing loss may occur. Symptoms may mimic Meniere's syndrome. Also, while migraine and its aura typically last hours, some patients have symptoms that can persist for days or weeks. In women, symptoms often (but not always) precede menstruation by a week. Migraine aura can be treated with dietary modification as certain foods, such as red wine, chocolate, strong cheese, fresh bread, or citrus, may trigger symptoms. If dietary modification does not resolve symptoms, medications are often used. Vascular Dizziness Maintenance of balance requires not only the input from the inner ears and other organs, but the brain and its neural connections must all be working prop- erly. If areas of the brain that assist in balance do not receive adequate blood supply, even temporarily, dizziness can occur.
Causes of vascular dizziness are varied. Arthritis in the neck can cause compression of arteries to the head, and cholesterol plaques may narrow these arteries too, causing decreased blood flow. Often, blood pressure to the brain can drop temporarily when standing up quickly, especially in the elderly and those who take blood pressure medication. Spe-cial imaging techniques such as MRI or Doppler may be needed to accurately diagnose these problems. Perilymphatic Fistula The inner ear is a fluid-filled bony maze within the skull. If fluid leaks from its bony casing, dizziness and hearing loss may occur. The leak usually arises from the oval and round window membranes, which are inherent areas of anatomical weakness. The leak may occur spontaneously, with heavy straining, or after trauma. Some children may be born with an abnormal connection between their brain and their ear, termed "Enlarged Vestibular Aqueduct". This can sometimes be detected on a CT scan and can lead
to fluctuating hearing loss as well as dizziness. Inner ear leaks may heal on their own with rest. In some cases, minor surgery is required to plug the leak. Superior Semicircular Canal Dehiscence Syndrome An unusual cause of dizziness is a hole involving the top of the superior balance canal. This hole can develop as a result of a weakness in the bone from birth or due to the pressure of the overlying brain that can wear away the bone. The hole allows ab- normal movement of the inner ear fluids resulting in dizziness often triggered by pressure to the ear canal, straining or loud sounds. Some patients may develop a conductive or mechanical hearing loss. Surgery may be indicated if symptoms are severe. tumors Rarely, tumors can be a cause of dizziness. The most common types are not cancerous. Acoustic neuro- mas are benign tumors of the balance nerve. They can cause unsteadiness, hearing loss, and tinnitus. MRI scans are used to identify these tumors. MEDICAL tREAtMEnt OF DIZZInESS
Reduction of Inner Ear Fluid Buildup Meniere's syn-drome can often be improved by reducing inner ear pressure. Decreasing the amount of sodium in the inner ear by curtailing salt in the diet combined with a water pill (diuretic) which eliminates the body's sodium are usually very effective. If you take water pills, make sure to have blood tests to ensure that potassium does not drop too low. Steroids are help-ful but have many side-effects. Make sure to discuss them with your doctor. Vestibular Rehabilitation To assist the body's ability to compensate for a balance loss, certain exercises can speed recovery. These exercises can strengthen the balance system, and thereby decrease symptoms. These exercises will benefit almost all patients with any type of dizziness. Inner Ear Injections For Meniere's syndrome and a few other uncommon ear disorders, "intratympanic injection" of medica- tions may provide some benefit. These medications include steroids to decrease inflammation, or gen- tamicin, which has special effects on the inner ear. Gentamicin has been used as a way of destroying the inner ear without surgery. In progressive treat- ments, it can destroy the balance portion of the inner ear, leading to fewer dizzy spells. Gentamicin treat- ments require several visits in which the medication is placed through a small hole created in the ear drum. Careful monitoring is necessary the effective amount for symptomatic relief may vary from person to person. Despite its benefits, unsteadiness and hearing loss can also result from Gentamicin. There is small risk that intentional perforation of the ear drum will not heal or may become infected. Other Occasionally patients derive benefit from the Meni- ett device (Medtronic) designed for use in Meniere's syndrome. Ask your physician if you are interested in more information. SuRgICAL tREAtMEnt OF DIZZInESS
Surgery may be needed to treat dizziness if medical treatment fails. Several types of operations are avail-able, depending on the cause of the dizziness. Not all procedures are options for every patient. Some
can only be offered in severe situations.
You and your doctor will need to decide on which therapy is best for you. Pros and cons must always be weighed whether treatment is medical or surgi-cal. Factors in consideration include hearing, age, health and the severity of disease. Surgical risks vary according to the procedure and the individual's age and preexisting health status. Most inner ear opera-tions require a general anesthetic and an incision behind the ear after shaving a small amount of hair. Any ear surgery carries potential risks to the impor-tant structures in the area, albeit minimal. These include hearing loss, tinnitus, dizziness, taste distur-bance, facial weakness, infection and bleeding.
Surgery performed adjacent to the brain adds addi-tional risks to life, brain and the surrounding nerves. In order to prevent a leakage of spinal fluid, patients who undergo clipping of the balance nerve may require a small amount of belly fat taken as a graft to seal the area underneath the incision. Endolymphatic Sac Decompression In Meniere's syndrome, the inner ear is under excess pressure. Inner ear fluid is normally made from the brain's spinal fluid and is absorbed by the endo- lymphatic sac. In Meniere's disease, the sac fails to perform adequately and excess fluid pressure results in dizziness, tinnitus and hearing loss. By removing the natural bony covering that sits over the endolym- phatic sac, pressure in the inner ear may be reduced, resulting in significant improvement of Meniere's symptoms.
In the past, a small tube was placed into the sac to drain fluid, but we have proven that the surgery is just as successful without a tube and minimizes the risk of hearing loss. As the sac is partially embedded in bone between the ear and the thick covering of the brain, a very slight risk of spinal fluid leak is pos-
sible. Although surgery is successful for most, some patients may not notice dramatic improvement. Ul-timately, the procedure carries a low risk of hearing loss, so it is often recommend as the first choice for surgically treating Meniere's disease. Vestibular nerve Section When dizziness is severe, but hearing is still good, cutting the balance nerve between the inner ear and the brain is very effective in eliminating vertigo while preserving hearing. This procedure requires general anesthesia and 2-5 days of hospitalization. Access is through a small hole in the skull behind the ear, thus hair shave is required and sometimes, a small piece of belly fat may be harvested to decrease the chance of spinal fluid leak. There is always some vertigo following the surgery which typically resolves after several days. Although the dizzy attacks are usu- ally completely eliminated, some may experience persistent unsteadiness. Usually, the opposite inner ear will compensate for this but a balance exercise program is essential. Occasionally, some people may get headaches following the surgery. As with any craniotomy, there is a small risk of infection (menin- gitis), leakage of spinal fluid, or headaches.
If a patient has good or decent hearing, then both vestibular nerve section and endolymphatic sac decompression may be reasonable options.
The sac operation is a comparatively more minor procedure aimed to relieve pressure within the inner ear. Cutting the vestibular nerve is more radical, as it removes balance function completely. Although sac surgery is not quite as effective as cutting the nerve, it avoids the many potential risks involved with working within the brain's cavity. Furthermore, it is the only surgery that may actually improve hearing in some patients, especially if performed early in the course of the disease.
Trying to decide between these two operations is a common problem. The nerve clipping surgery is one of the most successful treatments for Meniere's disease but there are surgical risks inherent to work-ing along the nerve's origin at the brainstem. Also, it does take some time to recover before the other ear compensates. Head exercises are important to help overcome unsteadiness.
Unfortunately, Meniere's disease can sometimes affect not one but both ears. There is even more reluctance to cut either balance nerve, and so a sac decompression is generally preferred. Posterior Semicircular Canal Occlusion This procedure is only performed for severe and prolonged cases of BPPV. In this procedure, the por- tion of the inner ear which is causing the dizziness is blocked off by plugging its canal with tissue or bone. This prevents the abnormal motion of inner ear crystals. It is very effective in relieving vertigo and generally carries a very low risk of hearing loss. Perilymph Fistula Repair In patients with a perilymph fistula, the inner ear fluid leak may need to be patched. The eardrum is lifted and the likely areas of leakage are sealed with tissue. Often the leak is microscopic and may not be readily visible. Symptoms usually improve over several weeks. Labyrinthectomy In severe cases of dizziness, labyrinthectomy can eliminate symptoms by complete removal of all the inner ear structures. It is a very successful cure for dizziness. However, the surgery results in total loss of hearing in the operated ear and therefore, it is generally performed when there is already poor hearing in the involved ear. Following surgery, ver- tigo usually resolves in several days. Although the
vertigo attacks are usually completely eliminated, there may be persistent unsteadiness. Usually, the remaining inner ear will compensate for this but a balance exercise program is essential. Repair of Superior Canal Dehiscence In cases where symptoms due to superior canal dehiscence are severe, surgical closure may be indicated. Repair is performed by creating a win- dow in the skull (craniotomy) made above the ear, or in some cases, through the mastoid. The brain is gently elevated to expose the problem area, and the hole above the balance canal is patched with bone materials. RISKS AnD COMPLICAtIOn OF SuRgERY FOR DIZZInESS Hearing Loss Further hearing impairment in the operated ear may occur following any of the procedures and is always expected following labyrinthectomy. Perforation of the ear drum can cause some hearing loss. tinnitus Tinnitus (head noise) usually remains the same as before surgery, but may worsen in some patients. If the hearing declines following surgery, tinnitus may likewise be more noticeable. taste Disturbance and Mouth Dryness Taste disturbance and dry mouth are not uncommon for a few weeks following surgery. In some instances, this disturbance may be prolonged. Weakness of the Face The facial nerve travels through the ear in close as- sociation with the hearing and balance nerves, the
inner ear and the mastoid. Temporary weakness of one side of the face is an uncommon postoperative complication of ear surgery, and may result from swelling of the nerve. Permanent paralysis of the face is extremely rare. Further management may be required in this situation, and eye complications could develop necessitating specialist care.
Spinal Fluid Leak Some of the operations described above may result in a temporary leak of spinal fluid (fluid surround- ing the brain). This leak is always closed prior to the completion of the surgery. On occasion, however, the leak reopens and further treatment or surgery may be required to stop it. Infection Infection is a rare occurrence following dizziness surgery. Should it develop, however, it could lead to meningitis (an infection of the spinal fluid) and may require antibiotics. Fortunately, this complication is very rare. Imbalance Certain procedures can cause permanent destruc- tion of inner ear function. This usually eliminates vertigo spells, but may lead to chronic imbalance. Usually this will improve with physical therapy, but may be permanent. It is more common when dizzy problems are caused by both ears. Labyrinthectomy, vestibular nerve section, and gentamicin treatments almost always involve at least a temporary period of imbalance. Hematoma A hematoma (collection of blood under the skin in- cision) develops in a very small percentage of cases, prolonging hospitalization and healing. Reoperation to remove the clot may be necessary if this occurs. Craniotomy For vestibular nerve sections, a craniotomy (open- ing the skull) is required. Although unlikely, leakage of spinal fluid is possible, however it is minimized by placing a plug of belly fat into the area. There is a slight risk of long term headaches (which can be treated with anti-inflammatory medications). Other very rare complications include meningitis, bleed- ing, stroke, or even loss of life.
Make sure to ask your doctor how soon you may return to work or driving after surgery. This will vary based on the severity of your dizziness, your job and the type of surgery. It may range from days to many weeks. Stuffiness and hearing loss can be expected for some time with any ear operation. This will usu-ally improve slowly as your body absorbs the healing fluids.
Fortunately, most types of dizziness can be cured or at least improved. But in some cases, no medical or surgical treatment may be effective. If so, patients will need to learn how to adapt to a chronic prob-lem. Diet, rehabilitation and exercise can all be important as can developing a positive attitude. An-tidepressants are sometimes very effective, not only to help with any anxiety and depression that may ac-company chronic dizziness, but also some of these medications can actually help the inner ear and brain's chemicals (neurotransmitters). These medica-tions should be supervised by your family doctor. higan Ear Institute Mic
and staff of the Michigan Ear Institute,
web site at www.michiganear.com Michigan Ear Institute higan Ear Institute (248) 865-4444 phone
Impact of Medical and Technological Advances on Survival Rates of People with Disabilities Disability Services Commission Contents Increase in life expectancy of people with disabilities 2.4 Cultural shifts and changes in medical practice 2.7 Awareness and accessibility of medical and technological 2.8 Specific needs of women with disabilities 2.10 Impact of economic ration
Preventive Veterinary Medicine 63 (2004) 237–256A meta-analysis of the milk-production responseafter anthelmintic treatment in naturallyJavier Sanchez , Ian Dohoo , Jeromy Carrier , Luc DesCˆoteaux a Department of Health Management, Atlantic Veterinary College, University of Prince Edward Island, 550 University Avenue, Charlottetown, PEI, Canada C1A 4P3 b Faculté de Médécine Vet
 The inner ear serves two main functions: hearing and balance. There are two types of hearing: mechanical and nerve (or electric). The mechanical part of hear-ing begins with a sound wave arriving at the outer ear, which then travels down the ear canal to vibrate the ear drum and a chain of three tiny hearing bones in the middle ear. The inner ear resembles a snail. The coil portion is the cochlea, which is responsible for the sensory part of hearing. Like a telephone, it converts sound energy into an electrical signal which is relayed through the hearing (cochlear) nerve to the brain.
The inner ear serves two main functions: hearing and balance. There are two types of hearing: mechanical and nerve (or electric). The mechanical part of hear-ing begins with a sound wave arriving at the outer ear, which then travels down the ear canal to vibrate the ear drum and a chain of three tiny hearing bones in the middle ear. The inner ear resembles a snail. The coil portion is the cochlea, which is responsible for the sensory part of hearing. Like a telephone, it converts sound energy into an electrical signal which is relayed through the hearing (cochlear) nerve to the brain.