L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Helios.hampshire.edu
See corresponding editorial on page 711.
Increased consumption of refined carbohydrates and the epidemicof type 2 diabetes in the United States: an ecologic assessment1-3
Lee S Gross, Li Li, Earl S Ford, and Simin LiuABSTRACT
1991 and 1999, and currently 60% of US adults are overweight
Background: Type 2 diabetes is an epidemic that is affecting an
(3, 7). These increases cannot be explained by the aging of the
ever-increasing proportion of the US population. Although con-
population alone, because similar increases are also being seen in
sumption of refined carbohydrates has increased and is thought to be
related to the increased risk of type 2 diabetes, the ecologic effect of
The cause of type 2 diabetes is multifactorial. Factors such as
changes in the quality of carbohydrates in the food supply on the risk
changes in exercise patterns and the ethnic composition of the US
of type 2 diabetes remains to be quantified.
population are likely contributors to the rising trends in diabetes,
Objective: The objective was to examine the correlation between
but there have been many debates in the scientific literature about
consumption of refined carbohydrates and the prevalence of type 2
the effects of specific dietary macronutrients on the risk of obe-
sity and type 2 diabetes (9 -12). Recent data suggest that a high
Methods: In this ecologic correlation study, the per capita nutrient
intake of refined carbohydrates may increase the risk of insulin
consumption in the United States between 1909 and 1997 obtained
resistance (13-16). Although an increase in the intake of refined
from the US Department of Agriculture was compared with the
carbohydrates in the form of processed grains, soft drinks, sweet-
prevalence of type 2 diabetes obtained from the Centers for Disease
eners, and refined flours in the US food supply has been reported,
scant quantitative data exist to determine whether such changes
Results: In a univariate analysis, a significant correlation with dia-
in dietary composition are related to the current epidemic of
betes prevalence was observed for dietary fat (r ҃ 0.84, P 0.001),
obesity and type 2 diabetes in the United States. To address this
carbohydrate (r ҃ 0.55, P 0.001), protein (r ҃ 0.71, P 0.001),
issue, we examined almost one century of dietary data and the
fiber (r ҃ 0.16, P ҃ 0.03), corn syrup (r ҃ 0.83, P 0.001), and total
history behind changes in the US diet. We conducted a multi-
energy (r ҃ 0.75, P 0.001) intakes. In a multivariate nutrient-
variate analysis of the correlation between changes in the prev-
density model, in which total energy intake was accounted for, corn
alence of type 2 diabetes and changes in dietary patterns in the
syrup was positively associated with the prevalence of type 2 dia-
betes ( ҃ 0.0132, P ҃ 0.038). Fiber ( ҃ Ҁ13.86, P 0.01) wasnegatively associated with the prevalence of type 2 diabetes. Incontrast, protein (P ҃ 0.084) and fat (P ҃ 0.79) were not associated
with the prevalence of type 2 diabetes when total energy was con-
We obtained estimates of the prevalence of type 2 diabetes in
the United States from the National Health Interview Surveys
Conclusions: Increasing intakes of refined carbohydrate (corn
maintained by the Centers for Disease Control and Prevention's
syrup) concomitant with decreasing intakes of fiber paralleled the
Diabetes Surveillance System (4, 17). Such data are available for
upward trend in the prevalence of type 2 diabetes observed in the
1935 and then annually beginning in 1957 and are based on
United States during the 20th century.
self-reports of having received a diagnosis of type 2 diabetes. In
1997, adoption of the type 2 diabetes diagnostic criteria of theWorld Health Organization effectively increased the prevalence
KEY WORDS
Type 2 diabetes, obesity, dietary fiber, refined
of type 2 diabetes in the United States after that year (18). We
carbohydrate, dietary carbohydrate, glycemic index
1 From the Inter-Medic Medical Group, North Port, FL (LSG); the De-
partment of Family Medicine, University Hospitals of Cleveland, Case West-
INTRODUCTION
ern Reserve University (LL); the Centers for Disease Control and Prevention,
Obesity and type 2 diabetes are occurring at epidemic rates in
Atlanta (ESF); the Division of Preventive Medicine, Brigham and Women's
the United States (1-3). From 1935 to 1996, the prevalence of
Hospital, Harvard Medical School, Boston (SL); and the Department of
diagnosed type 2 diabetes climbed nearly 765% (4). Currently,
Epidemiology, Harvard School of Public Health, Boston (SL).
16 million Americans have type 2 diabetes, one-third of whom
Supported by a CI-8 Clinical Investigator Award from Damon Runyon
do not even know that they have the disease (5). Recent data
3 Address reprint requests to LS Gross, Inter-Medic Medical Group, 2630
suggest that 47 million Americans have the metabolic syn-
drome-an insulin resistance syndrome that is associated with an
increased risk of type 2 diabetes (6). The prevalence of adult
obesity increased a staggering 57% in the brief period between
Accepted for publication November 6, 2003. Am J Clin Nutr 2004;79:774 -9. Printed in USA. 2004 American Society for Clinical Nutrition
REFINED CARBOHYDRATES AND TYPE 2 DIABETES
therefore excluded data from later than 1997. The diagnosticcriteria for type 2 diabetes also changed in 1979 (19). However,the rate of increase in the prevalence of type 2 diabetes actuallydecreased somewhat from the previous 2 decades after thischange in 1979, which suggested that the increase in prevalenceof diabetes beyond 1979 was not an artifact of that change. Thus,these data were included in our analysis.
The prevalence of obesity was based on the measured height
and weight of a random sample of the civilian noninstitutional-ized population aged ͧ 20 y, and is reported as a percentage ofthe US population with a body mass index (BMI; kg/m2) of ͧ 30. The data came from the National Health Examination Survey(NHES 1960 -1962); the first, second, and third National Healthand Nutrition Examination Surveys (NHANES I, 1971-1974;
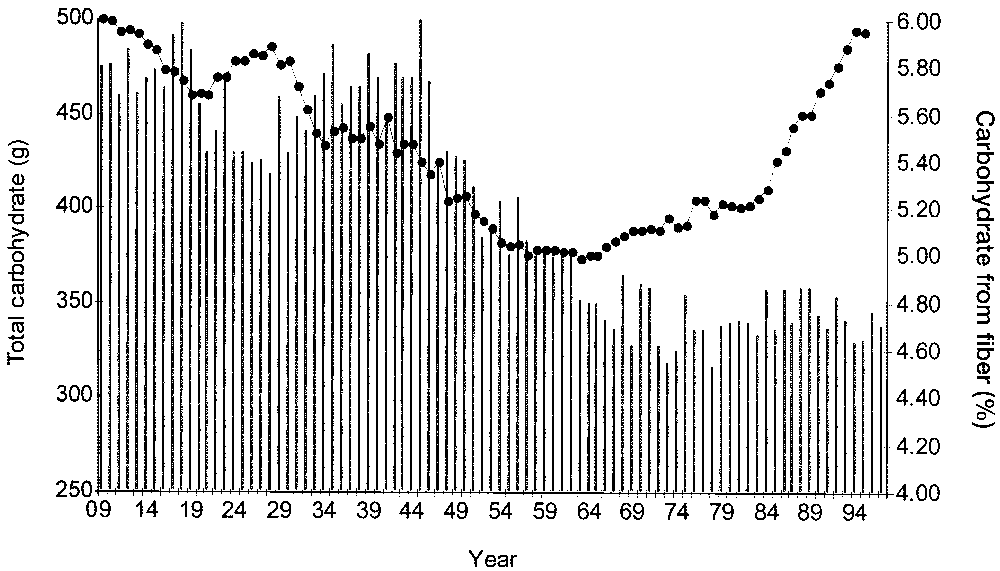
FIGURE 1. Change in total carbohydrate consumption (F) and the per-
NHANES II, 1976 -1980; NHANES III, 1988 -1994); and
centage of carbohydrate from fiber (vertical bars) in the United States be-tween 1909 and 1997 (17).
Unless stated otherwise, the nutrient content of the US food
supply and other nutrition data were obtained from the National
In a multivariate nutrient-density model (Table 1)-in which
Nutrient Data Bank, which is maintained by the Center for Nu-
total energy, corn syrup, fiber, fat, and protein intakes were
trition Policy and Promotion and the Economic Research Service
simultaneously included- corn syrup was positively associated
of the US Department of Agriculture (20). Nutrient data are based
with the prevalence of type 2 diabetes ( ҃ 0.0132, P ҃ 0.038),
on food disappearance and were calculated with the use of food
whereas dietary fiber ( ҃ Ҁ13.86, P 0.01) was negatively
availability data from the Economic Research Service and on the
associated with the prevalence of type 2 diabetes. In contrast, the
basis of the nutrient content of the edible portion of the available
percentages of energy from protein (P ҃ 0.083) and fat (P ҃
food supply as calculated by the Nutrient Data Laboratory of the
0.79) were not associated with the prevalence of type 2 diabetes
Agricultural Research Service. These food-composition data are
after adjustment for total energy intake and other dietary vari-
the numerical foundation of essentially all public and private
ables in the multivariate nutrient-density model.
work in the field of human nutrition (20).
Until 1980, the total energy intake remained relatively con-
Regression analysis was performed to examine the correlation
stant. Between 1980 and 1997, however, total energy intake
between macronutrient consumption and disease rates. A multi-
increased by 500 kcal/d. This increase was due primarily to
variate nutrient-density model was used to control for total en-
increases in dietary carbohydrate. Specifically, 428 kcal (nearly
ergy intake (21). In particular, corn syrup was selected to repre-
80% of the increase in total energy) came from carbohydrates, 64
sent refined carbohydrates in the model, because it is a highly
kcal (12% of the increase in total energy) came from protein, and
refined substance that is consumed in vast quantities in the
only 45 kcal (8% of the increase in total energy) came from fat.
United States in the form of soft drinks, commercial baked goods,
This represents a relative increase in consumption of dietary
ready-to-eat breakfast cereals, and many other commercially
carbohydrates from 48% to 54% of total energy intake over a
processed food products. Similarly, dietary fiber was selected
20-y period and a relative decrease in dietary fat from 41% to
because it generally is removed during the refining process. All
37% of total energy intake. During the same period, the preva-
P values are two sided. The statistical analysis was performed
lence of type 2 diabetes increased by 47% and the prevalence of
with the use of EPI-INFO (2002; Centers for Disease Control and
obesity increased by 80%, indicating a significant positive cor-
relation between the percentage of energy from refined carbo-hydrates and the prevalence of type 2 diabetes and obesity.
The total per capita use of caloric sweeteners increased by 86%
between 1909 and 1997, and the type of sweeteners used also
changed dramatically. Corn syrup sweeteners, which were al-
Dietary carbohydrate steadily decreased from 500 g/d in 1909
most nonexistent at the beginning of the century, now comprise
to 374 g/d in 1963, largely because of a decrease in the consump-tion of whole grains. Simultaneously, dietary fiber decreased at
a greater rate- by nearly 40%. Since 1963, the consumption of
Multivariate nutrient-density model for examining the associations
carbohydrates steadily increased back to 500 g/d; however, fiber
between trends in nutrients and the prevalence of type 2 diabetes in the
consumption did not increase proportionately. This finding re-
flects an increased consumption of refined carbohydrates over this time period (Figure 1). From 1963 to 1997, the consumption
of total fat increased nearly 30%, protein consumption increased
8%, and total energy consumption increased 9%.
In a univariate analysis of the available data for the period
between 1909 and 1997, a significant correlation with the prev-
alence of type 2 diabetes was observed for intakes of dietary fat
(r ҃ 0.84 P 0.001), carbohydrate (r ҃ 0.55, P 0.001), protein
1 A positive  coefficient indicates an increased risk of type 2 diabetes,
(r ҃ 0.71, P 0.001), fiber (r ҃ 0.16, P ҃ 0.027), corn syrup
whereas a negative coefficient indicates a decreased risk of type 2 diabetes.
(r ҃ 0.83, P 0.001), and total energy (r ҃ 0.75, P 0.001).
All values are adjusted for each other. Energy value used for fiber ҃ 4 kcal/g. FIGURE 4. Increasing prevalence of type 2 diabetes (vertical bars) in the
United States between 1960 and 1997 with increasing carbohydrate intake(F) (14, 17). FIGURE 2. Change in total carbohydrate consumption in the United
States between 1909 and 1997, reflected by the replacement of whole grains
ately to the increase in consumption of refined carbohydrates in
(smaller circles) with corn syrup (larger circles) (17).
the United States (Figures 4 - 6).
Our data also indicate that modern carbohydrates are consid-
20% of the total daily carbohydrate intake and 10% of the daily
erably different from those consumed before the beginning of the
total energy intake, which represents an increase of 2100%.
20th century and that the US food supply has become reliant on
These sweeteners have surpassed sucrose as the leading sweet-
highly refined carbohydrates as significant sources of energy.
ener in the US food industry and account for much of the rebound
The refining process has changed the composition and thus the
increase in carbohydrate consumption after the mid-1960s,
quality of carbohydrates (22). For example, processing whole
largely replacing the losses due to whole grains (Figure 2). There
grains into white flour actually increases the caloric density by
was a significant correlation between the percentage of carbo-
10%, reduces the amount of dietary fiber by 80%, and reduces
hydrate from corn syrup and the prevalence of type 2 diabetes
the amount of dietary protein by almost 30% (23). Refining
(r ҃ 0.85, P 0.001; Figure 3).
removes many of the main ingredients, leaving a dietary sub-
The multivariate nutrient-density model was modified to de-
stance that is nearly pure starchy carbohydrate with fewer nutri-
termine the "toxicity" of changing carbohydrate quality. This
model included total carbohydrate, the percentage of carbohy-
Corn refining in the United States began around the time of the
drates from corn syrup, and the percentage of carbohydrates from
Civil War with the development of cornstarch (25). In 1866, it
fiber. In this model, corn syrup and fiber-potential indicators of
was discovered that cornstarch could be converted to glucose,
carbohydrate quality-accounted for 18% of the variability in
and by 1882 the corn industry was manufacturing "refined corn
the prevalence of diabetes when the intake of total carbohydrate
sugar." The remainder of the corn plant (fiber, germ, and protein)
that was removed in the refining process was sold for animal feedor for the conversion to corn oil. Corn syrup technology advancedsignificantly with the introduction of enzyme-hydrolyzed prod-
DISCUSSION
ucts. In 1921, crystalline dextrose hydrate was introduced. The
In this ecologic analysis, in which national data from 1909 to
purification and crystallization of glucose meant that, for the first
1997 were used, we found a strong association between an in-
time, corn-based sweeteners could compete in some markets that
creased consumption of refined carbohydrates in the form of corn
had been the sole domain of the sugar industry. In the mid-1950s,
syrup, a decreased consumption of dietary fiber, and an increas-
the technology for commercially preparing low-conversion
ing trend in the prevalence of type 2 diabetes in the United States
products such as maltodextrin syrup was developed. The next
during the 20th century. Furthermore, our data are consistent inthat obesity and the prevalence of diabetes increased proportion-
FIGURE 3. Increasing prevalence of type 2 diabetes (vertical bars) in the FIGURE 5. Increasing prevalence of obesity [BMI (in kg/m2) 30;
United States between 1933 and 1997 with increasing per capita percentage
vertical bars] in the United States between 1960 and 1997 with increasing
of carbohydrate intake from corn syrup (F) (14, 17).
REFINED CARBOHYDRATES AND TYPE 2 DIABETES
Health Interview Survey are self-reported, many studies haveindicated excellent agreement between self-reported data anddata from medical records concerning a person's diabetes status(31-35). The issue of confounding with obesity, physical activ-ity, or both is challenging. Unfortunately, there is no uniformsource of consistent information about physical activity in theUnited States for the period studied. The Behavioral Risk FactorSurveillance Survey has only produced such data since the 1990s(36). Similarly, the first national obesity data were from the early1960s, which provide only 5 usable data points from the NationalHealth Examination Survey and NHANES studies since that
FIGURE 6. Increasing prevalence of type 2 diabetes (vertical bars) in the
time. Use of such scant data to control for obesity would lack
United States between 1966 and 1997 with increasing consumption of refinedgrains in the form of ready-to-eat cereals (F) (14, 17).
sufficient power to be meaningful. However, because obesity islikely an intermediary for the development of type 2 diabetes,control for this variable would likely negate the contribution of
development involved the enzyme-catalyzed isomerization of
any macronutrient. Thus, the control for obesity may be a case of
glucose to fructose. The commercial production of high-fructose
overadjustment. These potential confounders will hopefully be
corn syrup (HFCS) began in 1967, at which time the fructose
teased out by future prospective studies.
content of the syrup was Ȃ15%. Further research enabled the
Classifying foods according to the physiologic effects ob-
industry to develop a higher-conversion HFCS that had a fructose
tained directly from metabolic experiments is useful in under-
content of 42%. After a few more modifications, an HFCS with
standing the health effects of diets (37). Indeed, the concept that
a fructose content of 55% became the sweetener of choice for the
carbohydrates vary in quality is not new (ie, carrots are not the
soft drink and ice cream industries, and an HFCS with a fructose
same as cake) and appears to have important clinical signifi-
content of 90% became a frequent choice for use in "natural" and
cance. The glycemic index (GI) is a relative in vivo measure of
"light" foods. By 2002, HFCS sweeteners represented 56% of
the plasma glucose response to a standardized amount of carbo-
hydrate. The glycemic load (GL) is a product of the GI and the
The results of this ecologic study need to be interpreted in the
total amount of carbohydrate consumed, incorporating the ef-
context of the study's strengths and weaknesses. Ecologic stud-
fects of both the quality and quantity of carbohydrate intake. A
ies, such as observational studies of individual persons, are sus-
growing body of evidence suggests that a high dietary GL in-
ceptible to confounding. The so-called ecologic fallacy may oc-
creases the risk of obesity, glucose intolerance, dyslipidemia,
cur when inferences are made about individual persons on the
type 2 diabetes, and coronary heart disease (38 - 49).
basis of solely population-level data. Our analysis may also have
In several small-scale metabolic trials, refined grains have
been limited by the use of food disappearance data at the popu-
been shown to cause a significant increase in insulin secretion
lation level that are indirectly related to intakes at individual
and the postprandial glucose response (50 -54). In general, sub-
levels. To address these issues, our analyses used only
stituting high-fiber, low-GI foods for high-GI foods significantly
population-level variables (energy from macronutrients) to pre-
improves fasting insulin concentrations, the postprandial insulin
dict the only ecologic outcome (population-level prevalence of
response, glycemic control, and lipid profiles (55- 65). Corn
type 2 diabetes). Because we avoided inferences about individualpersons from population data, no cross-level bias should occur
syrup largely consists of the monosaccharide fructose, in contrast
(26, 27). Also, because we applied food disappearance data only
with sucrose-which is a disaccharide of fructose and glucose.
from within the United States and did not compare regional,
Fructose, unlike sucrose, has been directly linked to insulin re-
international, or ethnic group data, the bias, if any, would at least
sistance in small human and animal studies and has been impli-
be uniform for the same population. Although food disappear-
cated in every metabolic abnormality associated with the meta-
ance data are an indirect measure of individual consumption,
bolic syndrome (66 - 69). Corn syrup is now endemic in the US
these data have been calculated annually for more than a century,
food supply, which places an unprecedented biochemical evo-
making them the only consistent data available for identifying
lutionary pressure for processing fructose.
Several prospective cohorts have incorporated the concept of
To establish a causal diet-disease relation, however, one must
GI in assessing the relations between dietary carbohydrate and
examine evidence from a variety of sources and look for con-
the risk of type 2 diabetes. In the Nurses' Health Study, the
gruence between these sources (28). This is especially important
multivariate-adjusted relative risk of type 2 diabetes during 6 y of
when interpreting population-level analyses of macronutrient
follow-up was 1.37 (95% CI: 1.09, 1.71) for an increase in GI of
intakes because the specific effects of individual macronutrients
15 units and was 1.47 (95% CI: 1.16, 1.86) for extreme quintiles
and the generic effect of total energy intakes may not be evident
of dietary GL. Women with both a high dietary GL and a low
in individual-based studies with small sample sizes (29, 30). To
cereal fiber intake were at an even higher risk of type 2 diabetes
this end, such ecologic studies have advantages over population-
(relative risk: 2.43; 95% CI: 1.12, 5.27) (70). In the Health Pro-
based interventions for identifying potential diet-disease rela-
fessionals' Follow-up Study, the multivariate-adjusted relative
risk was 1.37 (95% CI: 1.02, 1.83) in 6 y of follow-up for extreme
Changes in diagnostic criteria and screening practices for type
quintiles of dietary GL and 2.17 (95% CI: 1.04, 4.54) for the
2 diabetes may limit the ability to determine the extent of effect
combination of a high GL and a low intake of cereal fiber (71). In
due solely to dietary changes. To reduce this bias, we excluded
the Iowa Women's Health Study, however, neither the GI nor the
data beyond 1997. Although prevalence data from the National
GL were related to the risk of type 2 diabetes in 6 y of follow-up,
although dietary fructose and glucose were significantly associ-
physiological basis for carbohydrate exchange. Am J Clin Nutr 1981;
Our analysis confirmed that during the past century, especially
15. Jenkins DA, Jenkins AL. The glycemic index, fiber, and the dietary
treatment of hypertriglyceridemia and diabetes. J Am Coll Nutr 1987;
the past 20 y, the American diet has undergone a dramatic
change. Furthermore, our data indicate that, during the same
16. Brand Miller J. Importance of glycemic index in diabetes. Am J Clin Nutr
period, type 2 diabetes has reached epidemic proportions, exert-
ing a substantial health burden on society. These population-
17. Centers for Disease Control and Prevention. Diabetes surveillance 1999.
level data are consistent with findings from metabolic and pro-
Atlanta: US Department of Health and Human Services, 1999.
18. Expert Committee on the Diagnosis and Classification of Diabetes Mel-
spective studies of individual persons, which suggest that the
litus. Report of the Expert Committee on the diagnosis and classification
intake of refined carbohydrates increases the risk of obesity,
of diabetes mellitus. Diabetes Care 1997;20:1183-97.
glucose intolerance, dyslipidemia, and type 2 diabetes. The risk
19. Keen H, Jarrett RJ, Alberti KG. Diabetes mellitus: a new look at diag-
of type 2 diabetes may be reduced by replacing refined carbo-
nostic criteria. Diabetologia 1979;16:283-5.
hydrates with low-GI carbohydrate sources and whole-grain,
20. US Department of Agriculture, Center for Nutrition Policy and Promo-
tion. Nutrient content of the U.S. food supply. Version current 29 May
high-fiber products. Further prospective randomized trials are
2003. Internet: http://147.208.9.134/ (accessed 3 February 2004).
necessary to determine the absolute effect of such an interven-
21. Willett WC. Nutritional epidemiology. 2nd ed. New York: Oxford Uni-
22. Food and Rural Economics Division, Economic Research Service, US
LSG was responsible for the concept and design of the study, acquisition
Department of Agriculture. A century of change in America's eating
of data, analysis and interpretation of data, drafting of the manuscript, and
patterns: America's fascination with nutrition. Food Rev 2000;23:32-7.
critical review of the manuscript for important intellectual content. LL and
23. Durtschi A. Nutritional content of whole grains versus their refined
SL were responsible for the concept and design of the study, the analysis and
flours. Walton Feed Company. February 5, 2001. Data source: USDA
interpretation of data, the drafting of the manuscript, the critical review of the
manuscript for important intellectual content, statistical expertise, and su-
24. Brand-Miller J, Wolever T. The glucose revolution: the authoritative
guide to the glycemic index. New York: Marlowe & Company Publish-
pervision. ESF was responsible for the concept and design of the study, the
analysis and interpretation of data, the drafting of the manuscript, the critical
25. Corn Refiners Association, Inc. History of corn refining in the U. S.
review of the manuscript for important intellectual content, and statistical
Version current 13 August 2002. Internet: http://www.corn.org/web/
expertise. None of the authors had any personal or financial interests in this
ca2000.htm (accessed 4 February 2004).
26. Susser M. The logic in ecological: II. The logic of design. Am J Public
27. Susser M. The logic in ecological: I. The logic of analysis. Am J Public
REFERENCES
1. Mokdad AH, Ford ES, Bowman BA, et al. Diabetes trends in the U. S.:
28. Tarasuk VS, Brooker A. Interpreting epidemiologic studies of diet-
1980 -1998. Diabetes Care 2000;23:1278 - 83.
disease relationships. J Nutr 1997;127:1847-52.
2. Mokdad AH, Ford ES, Bowman BA, et al. The continuing increase of
29. Wacholder S, Schatzkin A, Freedman S, Kipnis V, Hartman A, Brown
diabetes in the U. S. Diabetes Care 2001;24:412(letter).
CC. Can energy adjustment separate the effects of energy from those of
3. Mokdad AH, Serdula MK, Dietz WH, Bowman BA, Marks JS, Koplan
specific macronutrients? Am J Epidemiol 1994;140:848 -55.
JP. The spread of the obesity epidemic in the United States, 1991-1998.
30. Schwartz S. The fallacy of the ecological fallacy: the potential misuse of
a concept and the consequences. Am J Public Health 1994;84:819 -24.
4. Centers for Disease Control and Prevention, National Center for Health
31. Midthjell K, Holmen J, Bjorndal A, Lund-Lzarsen PG. Is questionnaire
Statistics, Division of Health Interview Statistics. Census of the popu-
information valid in the study of a chronic disease such as diabetes. The
lation and population estimates. Hyattsville, MD: Centers for Disease
Nord-Trondelag diabetes study. J Epidemiol Community Health 1992;
5. Harris MI, Flegal KM, Cowie CC, et al. Prevalence of diabetes, impaired
32. Heliovaara M, Aromaa A, Klaukka T, Knekt P, Joukamaa M, Impivaara
fasting glucose, and impaired glucose tolerance in U. S. adults. The Third
O. Reliability and validity of interview data on chronic diseases. J Clin
National Health and Nutrition Examination Survey, 1988 -1994. Dia-
33. Kehoe R, Wu SY, Leske MC, Chylack LT. Comparing self-reported and
6. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome
physician-reported medical history. Am J Epidemiol 1994;139:813- 8.
among US adults: findings from the Third National Health and Nutrition
34. Bush TL, Miller SR, Golden AL, Hale WE. Self-report and medical
Examination Survey. JAMA 2002;287:356 -9.
record report agreement of selected medical conditions in the elderly.
7. Centers for Disease Control and Prevention, National Center for Health
Am J Public Health 1989;79:1554 - 6.
Statistics, Division of Health Examination Statistics. Prevalence of over-weight and obesity among adults: United States, 1999. Data from the
35. Paganini-Hill A, Ross RK. Reliability of recall of drug usage and other
National Health and Nutrition Examination Survey. Hyattsville, MD:
health-related information. Am J Epidemiol 1982;116:114 -22.
Centers for Disease Control and Prevention, 1999.
36. US Department of Health and Human Services, Centers for Disease
8. American Diabetes Association. Consensus statement. Type 2 diabetes
Control and Prevention. Behavioral risk factor surveillance system sur-
in children and adolescents. Diabetes Care 2000;23:381-9.
vey data. Atlanta: Centers for Disease Control and Prevention, 2001.
9. Bray GA, Popkin BM. Dietary fat intake does affect obesity! Am J Clin
37. Heller RF. Hyperinsulinemic obesity and carbohydrate addiction: the
missing link is the carbohydrate frequency factor. Med Hypotheses
10. Willett WC. Dietary fat plays a major role in obesity: no. Obes Rev
38. Frost G. Glycaemic index as a determinant of serum HDL-cholesterol
11. Liu S, Willett WC, Manson JE, Hu FB, Rosner B, Colditz G. Relation
concentration. Lancet 1999;353:1045- 8.
between changes in intakes of dietary fiber and grain products and
39. Frost G. The relevance of the glycaemic index to our understanding of
changes in weight and development of obesity among middle-aged
dietary carbohydrates. Diabet Med 2000;17:336 - 45.
women. Am J Clin Nutr 2003;78:920 -7.
40. Liu S, Manson JE, Stampfer MJ, et al. A prospective study of whole-
12. Hu FB, van Dam RM, Liu S. Diet and risk of type II diabetes: the role of
grain intake and risk of type 2 diabetes mellitus in US women. Am J
types of fat and carbohydrate. Diabetologia 2001;44:805-17.
13. Liu S, Manson JE. Dietary carbohydrates, physical inactivity, obesity,
41. Jenkins DA, Jenkins AL. The glycemic index, fiber, and the dietary
and the "metabolic syndrome" as predictors of coronary heart disease.
treatment of hypertriglyceridemia and diabetes. J Am Coll Nutr 1987;
Curr Opin Lipidol 2001;12:395- 404.
14. Jenkins DJ, Wolever TM, Taylor RH, et al. Glycemic index of foods: a
42. Liu S, Manson JE, Stampfer MJ, et al. Whole grain consumption and risk
REFINED CARBOHYDRATES AND TYPE 2 DIABETES
of ischemic stroke in women: a prospective study. JAMA 2000;284:
of low-fat, high-carbohydrate diets on risk factors for ischemic heart
disease in postmenopausal women. Am J Clin Nutr 1997;65:1027-33.
43. Reaven GM. Role of insulin resistance in human disease. Diabetes 1988;
58. Chandalia M, Garg A, Lutjohann D, von Bergmann K, Grundy SM,
Brinkley LJ. Beneficial effects of high dietary fiber intake in patients
44. Liu S. Insulin resistance, hyperglycemia and risk of major chronic dis-
with type 2 diabetes mellitus. N Engl J Med 2000;342:1392- 8.
eases-a dietary perspective. Proc Nutr Soc Australia 1998;22:140 -50.
59. Frati Munari AC, Benitez Pinto W, Raul Ariza Andraca C, Casarrubias
45. Liu S, Willett WC, Stampfer MJ, et al. A prospective study of dietary
M. Lowering glycemic index of food by acarbose and Plantago psyllium
glycemic load, carbohydrate intake and risk of coronary heart disease in
mucilage. Arch Med Res 1998;29:137- 41.
US women. Am J Clin Nutr 2000;71:1455- 61.
60. Frost G, Leeds A, Trew G, Margara R, Dornhorst A. Insulin sensitivity
46. Liu S, Manson JE, Stampfer M, et al. Dietary glycemic load assessed by
in women at risk of coronary heart disease and the effect of a low
food frequency questionnaire in relation to plasma high-density lipopro-
glycemic diet. Metabolism 1998;47:1245-51.
tein cholesterol and fasting triglycerides among postmenopausal
61. Nobels F, van Gaal L, de Leeuw I. Weight reduction with a high protein,
women. Am J Clin Nutr 2001;73:560 - 6.
low carbohydrate, calorie-restricted diet: effects on blood pressure, glu-
47. Jacobs D, Meyer K, Kushi L, Folsom A. Is whole grain intake associated
cose and insulin levels. Neth J Med 1989;35:295-302.
with reduced total and cause-specific death rates in older women? The
62. Gutierrez M, Akhavan M, Jovanovic L, Peterson CM. Utility of a short-
Iowa Women's Health Study. Am J Public Health 1999;89:322-9.
term 25% carbohydrate diet on improving glycemic control in type 2
48. Schneeman BO. Use of glycemic index in predicting risk of coronary
diabetes mellitus. J Am Coll Nutr 1998;17:595- 600.
heart disease. Am J Clin Nutr 2000;71:1455- 61.
63. Golay A, Eigenheer C, Morel Y, Kujawski P, Lehmann T, de Tonnac N.
49. Liu S, Manson J, Buring J, Stampfer M, Willett W, Ridker P. A high
Weight-loss with low or high carbohydrate diet? Int J Obes Relat Metab
glycemic diet in relation to plasma levels of high-sensitivity C-reactive
protein in middle-aged women. Am J Clin Nutr 2002;75:492- 8.
64. Wright J. Effect of high-carbohydrate versus high-monounsaturated
50. Heaton KW, Marcus SN, Emmett PM, Bolton CH. Particle size of wheat,
fatty acid diet on metabolic control in diabetes and hyperglycemic pa-
maize, and oat test meals: effects on plasma glucose and insulin re-
tients. Clin Nutr 1998;17(suppl):35- 45.
sponses and on the rate of starch digestion in vitro. Am J Clin Nutr
65. Lewis SB, Wallin JD, Kane JP, Gerich JE. Effect of diet composition on
metabolic adaptations to hypocaloric nutrition: comparison of high car-
51. Stilling B, Mehlsen J, Hamberg O, Larsen JJ, Gram NC, Madsbad S.
bohydrate and high fat isocaloric diets. Am J Clin Nutr 1977;30:160 -70.
Effect of a new starch-free bread on metabolic control in NIDDM pa-
66. Elliott S, Keim NL, Stern JS, Teff K, Havel PJ. Fructose, weight gain,
tients. Nutr Metab Cardiovasc Dis 1999;9:98 -101.
and the insulin resistance syndrome. Am J Clin Nutr 2002;76:911-22.
52. Holt S, Brand Miller J, Petocz P. An insulin index of foods: the insulin
67. Dirlewanger M. Effects of fructose on hepatic glucose metabolism in
demand generated by 1000-kJ portions of common foods. Am J Clin
humans. Am J Physiol Endocrinol Metab 2000;279:E907-11.
68. Higashiura K. Alteration of muscle fiber composition linking to insulin
53. Ricardi G, Rivellese AA. Dietary treatment of the metabolic syn-
resistance and hypertension in fructose-fed rats. Am J Hypertens 1999;
drome-the optimal diet. Br J Nutr 2000;83(suppl):S143- 8.
54. Ludwig DS, Majzoub JA, Al-Zahrani A, Dallal GE, Blanco I, Roberts
69. Suga A. Effects of fructose and glucose on plasma leptin, insulin, and
SB. High glycemic index foods, overeating, and obesity. Pediatrics
insulin resistance in lean and VMH-lesioned obese rats. Am J Physiol
[serial online] 1999;103:e26.Internet: http://www.pediatrics.org/cgi/
Endocrinol Metab 2000;278:E677- 83.
content/full/103/3/e26 (accessed 4 February 2004).
70. Salmeron J, Manson JE, Stampfer MJ, Colditz GA, Wing AL, Willett
55. Jeppesen J, Chen YDI, Zhou MY, Schaaf P, Coulston A, Reaven GM.
WC. Dietary fiber, glycemic load, and risk of non-insulin dependent
Postprandial triglyceride and retinyl ester responses to oral fats effects of
diabetes mellitus in women. JAMA 1997;277:472-7.
fructose. Am J Clin Nutr 1995;61:787-91.
71. Salmeron J, Ascherio A, Rimm EB, et al. Dietary fiber, glycemic load,
56. Jeppesen J, Chen YD, Zhou MY, Wang T, Reaven GM. Effect of vari-
and risk of NIDDM in men. Diabetes Care 1997;20:545-50.
ations in oral fat and carbohydrate load on postprandial lipemia. Am J
72. Meyer KA, Kushi LH, Jacobs DR Jr, Slavin J, Sellers TA, Folsom AR.
Carbohydrates, dietary fiber, and incident type 2 diabetes in older
57. Jeppesen J, Schaaf P, Jones C, Zhou MY, Chen YD, Reaven GM. Effects
women. Am J Clin Nutr 2000;71:921-30.
REPRINT FROM NOVEMBER 27, 2008 BioCentury Vantia: New irons in the fire By Mike Flanagan company is hoping to settle on a once-daily Senior Writer Vantia Therapeutics Ltd. dosing regimen in its ongoing Phase IIa trial, Vantia Therapeutics Ltd. spun out of Ferring Pharmaceuticals A/S with a portfolio of small molecules that includes awith disease-modifying potential. The co
 REFINED CARBOHYDRATES AND TYPE 2 DIABETES
therefore excluded data from later than 1997. The diagnosticcriteria for type 2 diabetes also changed in 1979 (19). However,the rate of increase in the prevalence of type 2 diabetes actuallydecreased somewhat from the previous 2 decades after thischange in 1979, which suggested that the increase in prevalenceof diabetes beyond 1979 was not an artifact of that change. Thus,these data were included in our analysis.
REFINED CARBOHYDRATES AND TYPE 2 DIABETES
therefore excluded data from later than 1997. The diagnosticcriteria for type 2 diabetes also changed in 1979 (19). However,the rate of increase in the prevalence of type 2 diabetes actuallydecreased somewhat from the previous 2 decades after thischange in 1979, which suggested that the increase in prevalenceof diabetes beyond 1979 was not an artifact of that change. Thus,these data were included in our analysis.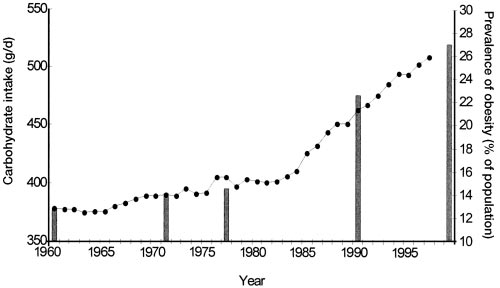
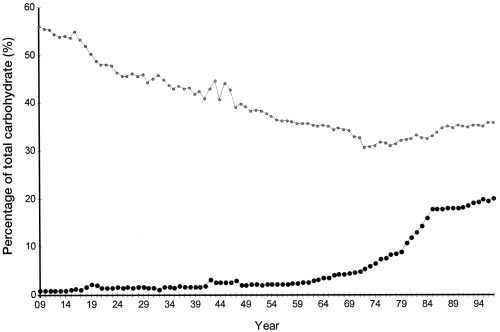
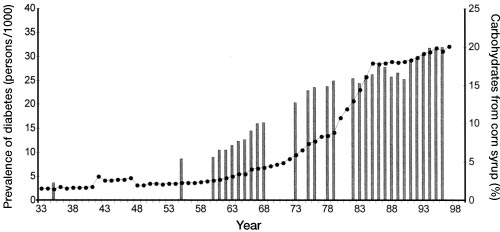
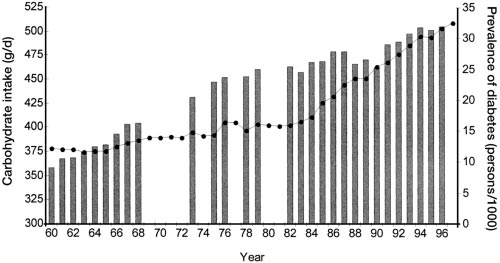 FIGURE 4. Increasing prevalence of type 2 diabetes (vertical bars) in the
FIGURE 4. Increasing prevalence of type 2 diabetes (vertical bars) in the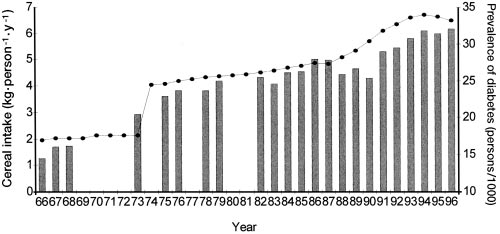 REFINED CARBOHYDRATES AND TYPE 2 DIABETES
Health Interview Survey are self-reported, many studies haveindicated excellent agreement between self-reported data anddata from medical records concerning a person's diabetes status(31-35). The issue of confounding with obesity, physical activ-ity, or both is challenging. Unfortunately, there is no uniformsource of consistent information about physical activity in theUnited States for the period studied. The Behavioral Risk FactorSurveillance Survey has only produced such data since the 1990s(36). Similarly, the first national obesity data were from the early1960s, which provide only 5 usable data points from the NationalHealth Examination Survey and NHANES studies since that
FIGURE 6. Increasing prevalence of type 2 diabetes (vertical bars) in the
REFINED CARBOHYDRATES AND TYPE 2 DIABETES
Health Interview Survey are self-reported, many studies haveindicated excellent agreement between self-reported data anddata from medical records concerning a person's diabetes status(31-35). The issue of confounding with obesity, physical activ-ity, or both is challenging. Unfortunately, there is no uniformsource of consistent information about physical activity in theUnited States for the period studied. The Behavioral Risk FactorSurveillance Survey has only produced such data since the 1990s(36). Similarly, the first national obesity data were from the early1960s, which provide only 5 usable data points from the NationalHealth Examination Survey and NHANES studies since that
FIGURE 6. Increasing prevalence of type 2 diabetes (vertical bars) in the although dietary fructose and glucose were significantly associ-
physiological basis for carbohydrate exchange. Am J Clin Nutr 1981;
Our analysis confirmed that during the past century, especially
15. Jenkins DA, Jenkins AL. The glycemic index, fiber, and the dietary
treatment of hypertriglyceridemia and diabetes. J Am Coll Nutr 1987;
the past 20 y, the American diet has undergone a dramatic
change. Furthermore, our data indicate that, during the same
16. Brand Miller J. Importance of glycemic index in diabetes. Am J Clin Nutr
period, type 2 diabetes has reached epidemic proportions, exert-
ing a substantial health burden on society. These population-
17. Centers for Disease Control and Prevention. Diabetes surveillance 1999.
although dietary fructose and glucose were significantly associ-
physiological basis for carbohydrate exchange. Am J Clin Nutr 1981;
Our analysis confirmed that during the past century, especially
15. Jenkins DA, Jenkins AL. The glycemic index, fiber, and the dietary
treatment of hypertriglyceridemia and diabetes. J Am Coll Nutr 1987;
the past 20 y, the American diet has undergone a dramatic
change. Furthermore, our data indicate that, during the same
16. Brand Miller J. Importance of glycemic index in diabetes. Am J Clin Nutr
period, type 2 diabetes has reached epidemic proportions, exert-
ing a substantial health burden on society. These population-
17. Centers for Disease Control and Prevention. Diabetes surveillance 1999.