L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Microsoft powerpoint - 01_clinicamp_26.04.2012.ppt [compatibility mode]
Waarom klinische farmacie vanuit de apotheek?
Q-Care = elektronisch voorschrijfsysteem (EVS)
Verpleging schrijft voor + arts valideert achteraf
Vanas = elektronische medicatiekasten op de afdeling
Inhoud: courante + dienstspecifieke medicatie (80%-regel)
A posteriori validatie Waarom klinische farmacie vanuit de apotheek?
UK / ideale wereld: 1 klinisch apotheker / 25 bedden
België: 1 FTE klinisch apotheker / 500 bedden?
"Full option" op 1 afdeling? "Light" voor heel het ziekenhuis? "Medium" voor enkele afdelingen? Clinical pharmacy "light" vanuit de apotheek: Hoe?
IZ, Neonatologie: geen Q-Care → geen controle 400-500 patiënten: wel controle
2 x daags validatie van alle elektronische medicatie-
opdrachten vanuit de apotheek Nieuwe opdrachten - Wijzigingen - Stopzettingen Gerangschikt per dienst + per patiënt +/- 1250 opdrachten per dag Voorbeeld Wat controleren we niet?
Infusen Standaard medicatie-schema's
Postoperatief pijnbeleid (≈ VAS-score) Materniteit
Veel gebruikte geneesmiddelen zonder (uitgesproken)
risicoprofiel Fraxiparine 0.3ml 1x per dag Amlor 5mg 1x per dag Tobradex oogzalf 2x per dag in linkeroog
1-malige opdrachten Chirurgisch of cardiologisch kortverblijf Wat controleren we wel?
Haldol 3 x 15mg per dag → 3 x 15 druppels per dag Floxapen 2 x 1g per dag (owv nierfct) → 4 x 1g per dag
Gentamicine 3 x 80mg per dag 8u-14u-20u → 8u-16u-24u
Keuze / allergie / nierfunctie / TDM Antibiogram: resistente kiem / (step-down)
VESanoid 1 x 10mg per dag → VESicare 1 x 10mg per dag Voordelen
(Tijds)efficiënte manier om "iets" te doen voor heel het
Snel capteren van individuele voorschrijffouten
Controle van een beperkt aantal parameters
Continuïteit Laagdrempelig voor andere collega's
IV → PO: selectief aantal GM, IV/PO-actiemaand, … Interacties: selectief aantal GM (voriconazole, rifampicine,…) FOCUS OP KLINISCH RELEVANTE ZAKEN!
Validatie van individuele medicatie-opdrachten, geen
therapie → geen zicht op het totale plaatje
→ geen opvolging/bijsturing als bv. nierfunctie verslechtert
Controle van een beperkt aantal parameters
Oppervlakkige screening
Klinische farmacie-items die niet aan bod komen:
Opname- en ontslagbeleid, medicatie-bevraging Afbouw / stoppen / opstarten van medicatie (IV → PO-switch) …
KF vanuit de apotheek vs. KF op dienst: een voorbeeld
Amoxiclav 3 x 2g iv op neurochirurgie Vanuit de apotheek:
• Controle nierfunctie: normaal, dus dosis + posologie ok • Controle antibiogram: geen kiem gekweekt • Controle allergie: peni-allergie!
Iom arts: start Ciproxine 2 x 500mg po (indicatie: pneumonie)
Op dienst: (ondertussen 7 dagen cipro)
Controle infectieparameters: flink gedaald!
Iom arts: Ciproxine nog 3 dagen verder (Tot.behandelingsduur: 10d)
Patiënt ziet er klinisch ook goed uit!
Iom arts: stop Lysomucil, stop Duovent
Title: Clinical Trial of Ceftriaxone in Subjects With Amyotrophic Lateral Sclerosis (ALS) Principal Investigator: Merit Cudkowicz, MD, MSc., Professor of Neurology, Harvard Medical School, Massachusetts General Hospital Contact: Sarah Titus, MPH (617) 726-1398 stitus@partners.org This trial is currently enrolling patients. Primary Outcome Measures: evaluation of multiple upper extremit
Current Health Care System Policy for Vulnerability Reduction in the United States of America: A Personal Perspective Edward J. Eckenfels Rush Medical College, Chicago, Ill, USA Aim. To raise questions about how the United States of America – which spends 1.3 trillion dollars on health care, con- ducts cutting-edge biomedical research, has the most advanced medical technology, and tr



 Waarom klinische farmacie vanuit de apotheek?
Waarom klinische farmacie vanuit de apotheek? 
 Waarom klinische farmacie vanuit de apotheek?
Waarom klinische farmacie vanuit de apotheek? 
 Clinical pharmacy "light" vanuit de apotheek: Hoe?
Clinical pharmacy "light" vanuit de apotheek: Hoe?

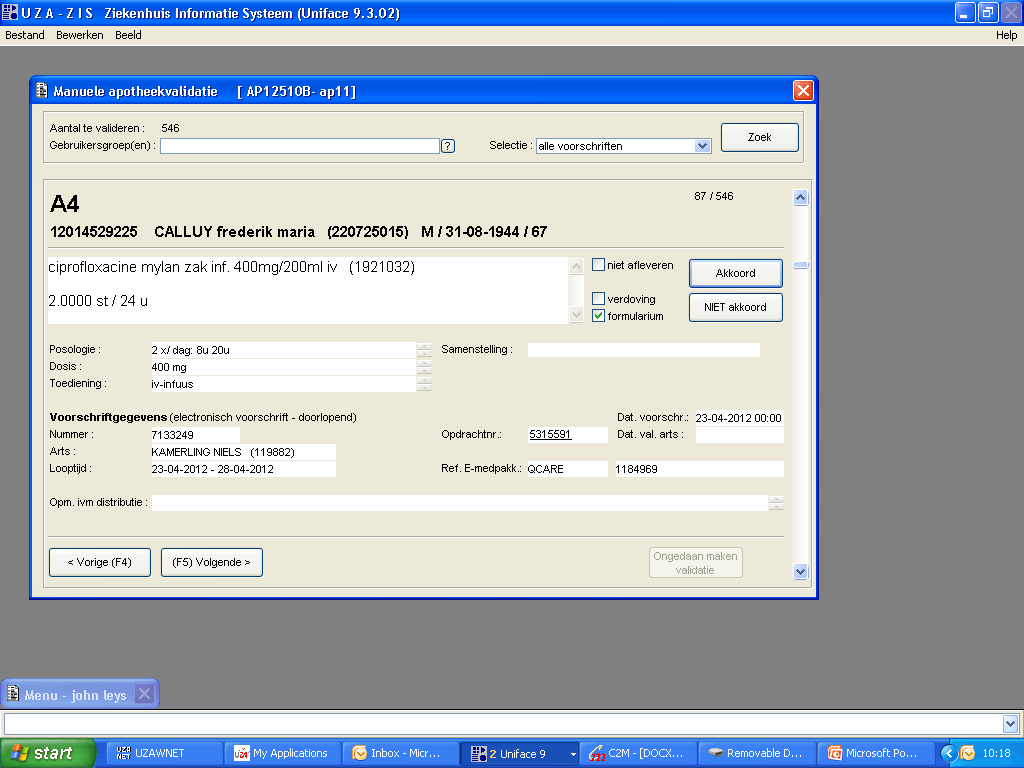 Voorbeeld
Voorbeeld
 Wat controleren we niet?
Wat controleren we niet?
 Wat controleren we wel?
Wat controleren we wel?
 Voordelen
Voordelen
 Validatie van individuele medicatie-opdrachten, geen
therapie → geen zicht op het totale plaatje
→ geen opvolging/bijsturing als bv. nierfunctie verslechtert
Controle van een beperkt aantal parameters
Oppervlakkige screening
Validatie van individuele medicatie-opdrachten, geen
therapie → geen zicht op het totale plaatje
→ geen opvolging/bijsturing als bv. nierfunctie verslechtert
Controle van een beperkt aantal parameters
Oppervlakkige screening
 KF vanuit de apotheek vs. KF op dienst: een voorbeeld
KF vanuit de apotheek vs. KF op dienst: een voorbeeld