L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Microsoft word - 1-8word
We are pleased to publish an offering from
our sister publication The Primary Care Companion to The Journal of Clinical Psychiatry about a topic of high importance to
all physicians. This special commentary is
Larry Culpepper. M.D.; Jonathan R. T. Davidson, M.D.;
the first independent project undertaken by
Allen J. Dietrich, M.D.; Wayne K. Goodman, M.D.; Kurt
Kroenke, M.D.; and Thomas L. Schwenk, M.D.
interests between psychiatry and primary
uicide is a tragic but not uncommon outcome to psychiatric illness.
The risk and rate of suicide among those who are mentally ill are
published in Prim Care Companion J Clin
higher than among the general population, and much effort has been
made by researches and clinicians in both psychiatry and primary care to
find ways to prevent suicide in these patients. However, reports that anti-depressant use can be associated with an increase in suicidal thoughts and behavior are cause for concern and have resulted in the public health
advisory issued by the U.S. Food and Drug Administration (FDA) in
March 2004. This advisory contained warnings relevant to 10 popular
antidepressant agents (Table 1): for a summary of the warning information
Issues Involved in the FDA's Assessment of
Drug Administration (FDA) issued a health
Whether Antidepressants Are Associated With Increased Suicidality Dr. Culpepper: Let me begin by posing some basic questions. What
are the issues involved in the FDA's assessment of whether antidepres-
depressants have been asked to include a
sants are associated with increased suicidality and potentially dangerous
warning statement on product labeling. This
behavior? What was this advisory based on, and why was it released now?
Dr. Goodman: This investigation started with a focus on the pediatric
population during the meeting of the FDA Psychopharmacologic Advi-
sory Committee and the Pediatric Subcommittee in February 2004. We
monitored for worsening of depression or
were presented with primarily unpublished data, particularly the results of
emergence of suicidal behavior. The full text
15 clinical trials of antidepressants in pediatric depression, that were sub-
mitted to the FDA. No child in those studies completed suicide. One might
expect that worsening depression led to suicidal behavior and that this
behavior would be more common in the placebo-treated groups, but that was not what was found. There was a stronger signal in some of the stud-
ies for suicidal behavior or suicide attempts, depending on how it was
defined, in the drug-treated groups compared with the placebo-treated
groups. This result was not uniform, however. In addition, in contrast to
what we see with adults, particularly with the selective serotonin reuptake inhibitors (SSRIs), the demonstrated improvement compared with pla-
cebo in this pediatric population was not large. In fact, only 3 of 15 studies
Primary Care Companion, assembled a
submitted to the FDA were considered positive. Others were either failed
Dr. Culpepper: In other words, there is a persistent trend that emerges
and advise clinicians how it will affect
from these data, although these data were not collected specifically to
Dr. Goodman: To put these events and findings in context, you have
to remember what happened more than 10 years ago with the1 report from Teischer and coworkers [Am J Psychiatry 1990:147:207-210] that
Faculty affiliations and disclosures appear at
raised concern about fluoxetine-induced suicidality in adults. Thereafter,
careful large-scale studies examined suicidality in fluoxetine-treated
Table 3. Symptoms of Activation Syndrome
Panic attacks Akathisia (severe restlessness)
Citalopram Mirtazapine a For more information about the advisory, go to
http://www.fda.gov.cder/drug/antidepressants/default.htm.
Dr. Culpepper: How did the FDA, expand its focus
from children and adolescents to include adults as well?
Table 2. Summary of Warning Information From
Dr. Goodman: The initial focus was clearly on the
the FDA Public Health Advisory__________________________
pediatric population. However, 63 public testimonials
Although no conclusion has been reached regarding the causal
were also presented at the meeting. These were anecdotal
relationship between antidepressant treatment and increased suicidality, health care providers should carefully monitor
reports, and the most typical ones were by bereaved
antidepressant-treated patients for worsening of depression or
parents talking about their teenaged or young adult child
emergence of Suicidality, especially at the beginning of treatment and after any change in dose
who had committed suicide shortly after starting
If depression worsens or suicidality emerges in an
antidepressant treatment. My speculation is that there
antidepressant-treated patient, health care providers should
was some influence from those anecdotal reports, which
evaluate the patient carefully to determine what intervention is needed (including stopping or changing the antidepressant
If you read the FDA advisory carefully, it does not
Activating symptoms (see Table 3) may be a signal of worsening
establish a firm, causal connection between suicidality
depression or increased suicidality in some patients. Health care providers should carefully evaluate any patient who develops these
and these antidepressants. There is also a focus on the
symptoms, especially if such symptoms were not pan of the original
so-called "activation syndrome," which may or may not
If an antidepressant medication needs to be discontinued, it should be
be a precursor to suicidal behavior. It may be that the FDA
realized that it needs to make all clinicians aware that pa-
Before starting a patient on antidepressant treatment, the health care
tients in all age groups may be sensitive to these drugs in
provider should carefully screen that patient for bipolar disorder
Health care providers need to educate patients and their families or
other caregivers to be watchful for worsening depression. emergence of suicidality, and activation symptoms and encourage
Activation Syndrome
them to report any changes to their health care provider
Dr. Culpepper: From both psychiatric and primary
To see the complete advisory, go to http://www.fda.gov/cder/drug/ amidepressants/default.htm and click on "Public Health Advisory."'
care perspectives, is the concept of an activation syn-drome new, or are prior concerns being repackaged (Table 3)?
patients [Leon AC, et al. Am J Psychiatry 1999:156: Dr. Dietrich: Thinking back to the age before SSRIs, 195-201; Khan A, et al. Int J Neuropsychopharmacol
I remember in medical school being told that when you
2001:4:113-118: Storosum JG, et al. Am J Psychiatry
prescribe an antidepressant, you had to monitor the pa-
2001;158:1271-1275], and any suspected relationship
tient very carefully during the initial phases of treatment.
was largely debunked. The difference now is the relative
The effects of the antidepressant would sometimes allow
strength of the pediatric data. We needed to consider
patients the motivation and energy to act on an impulse or
these data seriously and not just harken back to the previ-
desire that their depression had previously kept them
from acting on. This activation syndrome seems similar
One result to consider is that the signal of suicidal be-
but with increased specificity and a new label.
havior was higher in drug-treated patients than
Dr. Davidson: I agree to some extent. Even before
placebo-treated patients in some of the 15 studies
SSRIs, we were told to be careful in the first week or two
presented. It was not a consistent effect by any means. In
of antidepressant treatment, including electroconvulsive
fact, the risk ratio was elevated in only 3 of the studies.
therapy. The activation preceded the improvement of de-
Data from 25 pediatric studies were analyzed,
pressed mood and suicidal thoughts, so suddenly patients
comprising more than 4000 patients and including the J5
had the energy to carry out things that they had been
depression studies and 1 other depression study, 4
somewhat inhibited from doing because of retardation or
obsessive-compulsive disorder studies, 2 generalized
anxiety disorder studies. 2 attention-deficit/hyperactivity
There are a couple of factors to consider. Oneis that
disorder studies, and 1 social anxiety disorder study. In
any antidepressant treatment may, in the early phases,
all, 109 patients experienced 1 or more events that were
provoke suicidal behavior, but that doesn't really answer
considered "possibly suicide related."
the problem under discussion, because these reports of
self-destructive behavior are not all early side effects.
which we have all seen for the entire time we have been
They seem to be scattered throughout the entire period of
working with patients. This advisory does return our fo-
cus to close follow-up and monitoring as well as making
A second observation is that we have definitely known
appropriate adjustments when treating depressed patients,
for some time about what used to be called the
but I am unconvinced that antidepressants regularly trig-
antidepressant jitteriness syndrome. I have seen this
ger some ominous, discrete event that spins into a high
syndrome more in patients with panic disorder or
somatizing anxiety; these patients may get very agitated and then become distressed by that agitation. In my
Management of Patients
experience, they do not often become suicidal. Overall, if
Already Taking Antidepressants
you see a patient with these symptoms, you have to
Dr. Culpepper: We all have patients of a variety of
determine if there may be complicating symptoms of
ages who are taking antidepressants, and many of them
panic attacks or unrecognized anxiety, or, for that matter,
have probably heard the news reports about the FDA ad-
patients with undiagnosed bipolar disorder. These issues
visory and other news stories about suicide and antide-
are of some concern in determining what is meant by
pressants. The advice from the FDA is that concerned pa-
tients should call their physicians-we are the physicians
Dr. Culpepper: I was perplexed about the activation
in question, so what do we tell patients who are concerned
syndrome because as I read the FDA's description of
symptoms (see Table 3). I was reminded of an idiosyn-
Dr. Schwenk: Early, close follow-up has always been
cratic reaction that I have seen in some patients-for ex-
recommended but has not always been done as it should
ample, an anxiety patient started on treatment with
be. We must take these issues seriously and remember that
full-dose fluoxetine who comes in for a follow-up visit
these are powerful medications used to treat a powerful
pacing and reporting inability to sleep. In other words, I
disease. However, what primary care physicians do well
are substantive and detailed discussions of side effects
Dr. Goodman: I think for the most part, the committee
and functioning. We need to have these discussions with
was talking about early side effects on the basis of clinical
our antidepressant-treated patients as often as necessary
impressions, including the anecdotal reports of parents in
until we-doctor and patient-are both convinced
which suicide seemed to be a problem in the early phases
of the treatment. If this is the case, it would coincide with
Dr. Culpepper: It does seem like we have moved
what Drs. Davidson and Culpepper mentioned, the need
from a time when a new patient with depression came
to be careful with the anxious patient and to start such a
in weekly at the beginning of treatment to now, when
patient with a low dose, monitor carefully, and raise the
we will telephone a new patient for follow-up and then
see that patient in the office 3 or 4 weeks after initiating
In addition, multiple mechanisms might account for
treatment, if not up to 6 or 8 weeks. Is this a wake-up call
this activation syndrome or behavioral toxicity. In fact,
that our treatment paradigm may have gotten too slack?
during the 1991 committee meetings that followed
Dr. Kroenke: With the older antidepressants, I think
Teischer and coworker's original report on
part of the reason that we might have had them return ear-
fluoxetine-induced suicidality. Dr. Teicher presented a list
lier was often for something other than monitoring for ac-
of possible mechanisms to explain suicidality. An
tivation. We had to titrate the older drugs more often, and
example is the rollback phenomenon, which is an older
the newer ones have lulled us into thinking that one dose
term that describes a patient with melancholic depression
may fit all and, even if it does not, we usually find we
or psychomotorically retarded depression who becomes
need to adjust the dosage less often. Second, the older
activated after treatment. However, the committee felt
agents are toxic and possibly lethal if overdosed, so we
that this phenomenon probably occurs rarely in the
were very cautious in following up with new patients and
pediatric population, in which few depressed children are
gave them limited amounts of the drug. The SSRIs and
psychomotorically retarded. Another item on this list is
newer antidepressants have decreased a lot of that fear of
stage shifts from depression to mixed or manic states in
patients with undiagnosed bipolar disorder.
Dr. Dietrich: Doling the medicine out carefully was Dr. Culpepper: Other mechanisms on that list are
certainly much more a part of my practice with the
paradoxical worsening of depression, akathisia, and
tricyclic antidepressants (TCAs) than it is with the
insomnia, in addition to induction of anxiety and panic at-
SSRIs. I have also found that my patients are less
tacks. The activation syndrome, then, may cover a set of
interested in coming back for an office visit 1 or 2 weeks
behaviors that may have several different origins.
after starting an antidepressant. Many of these patients are
Dr. Schwenk: We are dealing with a very loosely
managing to work in spite of the depression and are
defined and heterogeneous group of problems, many of
Table 4. Timeline of Regulatory Action on Antidepressants in
event was the decision by the regulatory body in the
United Kingdom to contraindicate or discourage the use
The Medicines and Healthcare Products Regulatory Agency
of all SSRIs except fluoxetine in the pediatric population.
(MHRA) in the United Kingdom issued a warning
The reason given was that few data supported the use
about the use of paroxetine in children younger
of these agents in children, and therefore the risk-benefit
The FDA recommends that paroxetine not be used
ratio was unfavorable. In a sense, the decision that the
in children or adolescents due to increased risk
FDA came to was a compromise that indicated that, on
one hand, they realized there are insufficient data to es-
Labeling for venlafaxine changed to clarify that the
tablish a direct connection between these medications
agent is not recommended for use in children;
"Dear Health Care Professional" letter sent by
and suicidality, yet on the other hand, they also realized
that there has been insufficient attention paid to some of
MHRA advised against the use of venlafaxine in
the early side effects of antidepressant treatment that may
ormay not be precursors to suicidal behavior.
MHRA advised against the use of a l l SSRIs except
fluoxetine in children: paroxetine. venlafaxine
One of the presentations made at the February
sertraline, citalopram, and escitalopram are
2004 FDA meeting was by David Shaffer, F.R.C.P.,
contraindicated in this age group, while the use of
F.R.C.Psych. He presented suicidal trend data for the
adolescent population and showed very clearly a reduc-
Committee and the Pediatric Subcommittee of the
tion in suicide from1995 to 2000, the period in which
Ami-Infective Drugs Advisory Committee held a
SSRIs became the first-line treatment for depression
public meeting to review data and reports of
(Ftgure1). The introduction and increased use of SSRIs
antidepressant-induced suicide in children and
may not solely account for this decrease, but Dr. Shaffer
FDA issued a public health advisor) warning
was unable to exclude them as contributing to the lower
clinicians to observe child and adult patients
suicide rate (go to http://www.fda.gov/ohrms/dockets/
closely to monitor for worsening depression and/or suicidality.
ac/04/slides/4006S l_03_Shaffer.htm to view the slide
Abbreviations: FDA = U.S. Food and Drug Administration.
SSRI = selective serotonin reuptake inhibitor.
Overall, even in the pediatric population, these drugs
have done more good than harm and have saved lives. However, a cautionary note is warranted to remind physi-
work again so soon after the first office visit. Williams
cians, patients, and family members that some
and colleagues conducted a national survey of primary
patients-children in particular-have adverse behavioral
care physicians and discovered that the average time to
reactions in the early phases of treatment. Everyone
follow-up visit was almost a month for patients with
involved in the patient's care and treatment should look
major depression and longer than a month for patients
out for these reactions and the physician should alter
with dysthymia and minor depression [Arch Fam Med
the treatment as needed-adjust the dose of the
1999:8:58-67]. For whatever reason, follow-up visits
medication, stop the medication, or add another
occur less often than many of us would like to see.
Dr. Kroenke: One thing that confused me is that the Dr. Culpepper: Let us narrow this down to some
FDA is recommending a label change for these 10 newer
pragmatic advice. One of your patients who have been
antidepressants (see Table 1) but not for the older agents
taking an antidepressant for some time asks you. "I've
such as the TCAs. Does this mean that the FDA considers
read this stuff in the newspaper: should I stop taking my
this issue of activation irrelevant with the TCAs? Another
antidepressant?" What do you tell him or her?
question is how do you separate common initial side ef-
Dr. Schwenk: I would first ask the patient if he or she
fects of an antidepressant, which many of these symptoms
has been experiencing any of the side effects or symp-
that we have discussed are, from an actual syndrome that
toms that are described in the health advisory. If so, I
would ask the patient to come in so that we can assess the
Dr. Davidson: This advisory started with data on
situation. If not, reassurance is all that is necessary.
children, and my impression is that TCAs are used in-frequently in children because of some of the earlier stud-
Management of Patients
ies showing cardiovascular risks. These agents certainly
Who Need Treatment With an Antidepressant
should have been included in the FDA advisory, which
Dr. Culpepper: Let us move on to discuss patients
who need treatment with an antidepressant. For example,
Dr. Goodman: The FDA's action in issuing the health
you evaluate a patient who scored a 20 on the depression
advisory was of course preceded by the action of the
section of the Patient Health Questionnaire (PHQ-9),
British counterpart to the FDA (Table 4), The seminal
which indicates severe depression, but who has never re-
ceived antidepressant treatment. How do you proceed?
Figure I. Changes in Youth (aged 15-24 years) Suicide Rates in the United States During the 20th Century"
"Modified from David Shaffer's slide presentation "Suicide and "Related Problems in. Adolescents," given at the Feb. 2.
2004,meeting of the Psychopharmacologic Advisory Committee and the Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee of the U.S. Food and Drug Administration [FDA]. Available on the FDA Web site at: http://www.fda.gov/ohrms/dockets/ac/04/slides/4006S l-03-Shaffer.htm.
Dr. Kroenke: I would have a conversation with the pa-
Table 5. Questions to Ask Depressed Patients Who Express Suicidal Thoughts __________ ___
tient that focuses specifically on suicidality, rather than a
Have you made a plan for committing suicide?
broad array of symptoms, to determine whether he or she
How seriously are you thinking about it?
had thoughts of death or dying and active thoughts about
What is stopping you from committing suicide?
planning it-in other words, I would try to determine
Do you have weapons in your home? What kind of emotional support system do you have?
if there was risk of suicidality. I would have this discus-sion on the day treatment begins. The higher the risk, the more likely it would be that I would involve mental health
Managing Antidepressant-Treated Patients Who Report Increased Suicidality Dr. Culpepper: What if, when you inquire about sui- Dr. Culpepper: From a psychiatrist's perspective,
cidality, the patient says, "Oh no, I would never do that.
how would you now handle referrals from primary care
I haven't had any serious inclination that way." Do you
physicians of depressed patients who have become sui-
simply start medication treatment? Do you now, since the
cidal? For example, let us say that I have a patient who
advisory, want to get a written consent before starting
one day remarks to me that she has been thinking about
medication? What do you tell the patient about the FDA
suicide, that one of her aunts committed suicide by over-
dosing on pills, and that that option is looking appealing
Dr. Dietrich: If I am satisfied that the suicide assess-
to her. I refer her for psychiatric consultation. What are
ment is negative and that the patient has neither passive
you going to do as my psychiatric consultant for this pa-
nor active thoughts of death at this time, I would next
tient? In particular, how might you deal with her differ-
go into the business of patient preferences-whether the
patient prefers a counseling approach or a medication
Dr. Davidson: First, I would be sure to do a careful
approach. Assuming that the patient prefers medication
evaluation of suicide risk (Table 5). If there appears to be
either alone or in addition to counseling, I would review
a fairly serious risk, I would consider hospitalizing the pa-
side effects, as usual, but now I would call the patient's
tient or at the very least entering into a contract with her in
attention to the recent FDA warning and tell him or her
which she promises not to commit suicide and to call me
what symptoms to watch out for. I would inform the pa-
or another person if and when Serious thoughts about it
tient that, for this reason, I will be monitoring his or her
cross her mind. If the risk does not seem acute, then I
response to medication closely, and I would also ask the
would tell her that she needs immediate treatment. The
patient to touch base with me the following week.
more suicidal the patient is, the more compelling the case
help prevent this tragic outcome. We all-psychiatrists
for prescribing a medication as opposed to counseling, in
and primary care physicians alike-must be careful in the
my opinion, I would talk about the medications with her
early phases of treatment, particularly when treating chil-
and say. "You probably have heard about the concerns in
the media and from the FDA about whether these drugs can make you more suicidal, and in my judgment, it is un-
Managing Antidepressant-Treated Patients
likely to happen." I would reassure her that it is more
Who Report Activation Syndrome
likely that she will improve with antidepressant treatment,
Dr. Culpepper: What about patients who report not
but that we would need to stay in close contact, especially
overt suicidality but symptoms of activation syndrome?
during the first few weeks of treatment. I would also in-
For example, what course of action do you take with a
volve a spouse, family member, or close friend in her care
patient who has been taking an antidepressant for 2 weeks
to make sure someone is always available as support.
and who calls you to report feeling unbearably on edge
Dr. Culpepper: What if the patient is a 16-year-old
boy with some symptoms of obsessive-compulsive disor-
Dr. Schwenk: Assess suicidality and make a decision
der and other anxiety in addition to the suicidal thoughts?
on that basis. If the patient has been on treatment for only
Dr. Goodman: Dr. Davidson's answer was compre-
2 weeks, I would probably tell him or her to stop taking
hensive, but I would add that with a patient with anxiety,
the medication and see me as soon as possible.
it may be wise to start at a lower dosage than you nor-
Dr. Culpepper: Would anybody taper medication?
mally would in depression without a concomitant anxiety
Dr. Goodman: It might be only necessary to lower the
disorder. I would also warn patients like this that they
dose. That is an individual decision, whether to stop treat-
might feel a little bit anxious or jittery when they first start
ment or taper the dose. You should not increase the dose at
the medication and that they should call me if they feel
uncomfortable. This is assuming that I have come to some
It seems somewhat analogous to the situation of differ-
sort of agreement with them, as Dr. Davidson recom-
entiating akathisia from worsening of psychosis-you
mended, and that they can be maintained on an outpatient
cannot assume that the symptoms represent a worsening
of the underlying condition without first testing to see if
With an adolescent, we also need to realize that the
they are due to the medication. You conduct this test by
efficacy of these agents may be different. The thrust of the
stopping the medication, adding an adjunctive agent, or
regulatory action in the United Kingdom, after all, was
lowering the dose of the original medication.
that the data demonstrating the efficacy of the SSRIs
Dr. Culpepper: In the primary care setting, how do we
(except fluoxetine) in younger patients were weak or non-
differentiate this activation syndrome in an
existent. It was that lack of evidence that made the
antidepressant-treated patient from undiagnosed bipolar
risk-benefit ratio weighted more on the risk side, given
disorder? Symptoms of activation syndrome seem similar
the signals of suicidal behavior in this age group. A
to those of antidepressant-induced mania or rapid cycling.
recent article reviewed those data, published and
Is that a diagnostic issue that we can deal with in primary
unpublished, in more detail [Whittington CJ, et al. Lancet 2004:363: 1341-1345].Dr. Schwenk: A key point here is that primary care
When treating adolescents, it is also important to re-
physicians like myself must become more expert in the
member that they may not be as effective as adults in verbalizing their experiences. They may feel
diagnosis and treatment of patients with bipolar disorder,
uncomfortable or anxious but unable to describe those
which has become much more prevalent in ourpractice
sensations adequately. I think you need to go out of your
than it used to be. In the past, most patients with bipolar
way with adolescents to urge them to contact you early in
disorder were referred to a mental health specialist, but
the stages oftreatment-even before their next office
now, for a variety of reasons, many are being treated by
visit-if they feel worse in any way, and then it will be
primary care physicians. I try to be much more attentive
your job to determine whether those feelings indicate
to these symptoms of agitation, irritability, and
worsening depression or are side effects of the
medication. My suspicion is that some young adults and
Dr. Dietrich: When I initiate treatment with an antide-
children have considered or even committed suicide
pressant, I try to gather a careful history in terms of both
because they did not have a way of understanding that
the patient's own previous episodes that might have been
what had happened to them was a result of negative
hypomanic and family history. I warn at-risk patients to
effects of the drug. Perhaps if we can share more
be watchful for these symptoms, and when I see a patient
information with young patients to help them recognize
who appears to be switching into a manic episode, 1 have
that unpleasant sensations and feelings might be
the luxury of getting a quick psychiatry consultation that
many primary care physicians may not have. 1 can easily get help from one of my psychiatry colleagues in sorting
out whether a patient may be on the verge of a bipolar
especially if these informants are educated about the ill-
ness and asked to watch out for certain types of changes.
Dr. Culpepper: What about the primary care physician
who has few if any opportunity for psychiatry consultations,
Concluding Thoughts
for example, a doctor who works in a rural area and may be
Dr. Davidson: One point that we need to make is the
a hundred miles from the nearest psychiatrist? What are
fact that there are good trials in children and adolescents
other possibilities for managing a patient who is
with anxiety disorders-obsessive-compulsive disorder,
experiencing activation symptoms? Would you ever think
social phobia, and generalized anxiety disorder-that
about prescribing atypical antipsychotics to this type of
have reported a positive signal in favor of the efficacy of
the newer antidepressants. There is virtually no evidence
Dr. Schwenk: Absolutely. We as primary care physi-
from the available database that the incidents mentioned
cians have to be much smarter about using mood stabiliz-
in the FDA advisory have taken place in the anxiety popu-
ers and atypical antipsychotics and not be as averse to us-
lation. We need to keep this very much in mind because
we are obligated to help our teenaged patients who de-
Dr. Culpepper: Would you consider ordering a toxicol-
ogy screen in this type of patient? I have seen patients with
Dr. Kroenke: I am concerned about generalizing
increased irritability and agitation who denied using alco-
study results and treatment strategies regarding
hol or illegal drugs, but their toxicology results were
children to adults and vice versa. For example, it may be
positive for cocaine, which of course can explain those
easier to involve an informant with a young patient whose
symptoms. Has anyone else had that experience?
parents are involved in every level of treatment. With an
Dr. Davidson: In many of the clinical scenarios we
adult patient, however, you often see the patient as an
have discussed, we need to make sure that the patient is
adult alone. The logistics of trying to contact a family
avoiding alcohol and illegal drugs. I have certainly seen
member to participate in treatment and negotiate the
patients who have appeared to be irritable and impulsive
and then discovered that they have mixed alcohol with
Dr. Culpepper: Those are both good points. When
their medication. We should always inquire about alcohol
I think about suicidality, I am reminded of the Institute of
Medicine's report on preventing suicide [http:// Dr. Culpepper: Earlier in the discussion, we touched on www.iom.edu/report.asp? id=3843]. One of the points in
contracting for safety. Does the FDA advisory about ac-
that report is that depression is often in the background of
tivation and suicidality alter your perspective on the
suicidal behavior, but that anxiety is often there as well.
effectiveness of contracting for safety?
Two other critical ingredients that heighten the risk of sui-
Dr. Schwenk: I believe that contracting is something
cide are impulsivity and substance abuse, which become
that primary care physicians have been taught to have
quite lethal when combined. How can clinicians quickly
some faith in, but my sense is that psychiatrists may not
Dr. Dietrich: With patients whom I have been treating Dr. Culpepper: I have been unable to pinpoint any sci-
for years and see fairly often, I have an intuitive sense
entific evidence that said that contracting works or does not
of their baseline level of impulsive behavior and can de-
work. Is it something that is unique to primary care, as Dr.
tect changes. The challenge comes with a new patient who
may evoke some concern in this area. In that case, I would
Dr. Goodman: I have some hesitations about contract-
ask many of the same assessment questions that Dr.
ing. If you accept the possibility that in some individuals,
Davidson suggested (see Table 5), about emotional sup-
by whatever mechanism, these medications can induce a
port systems, use of drugs or alcohol, and availability of
state change, then you have to wonder how good a safety
firearms and other means of harming oneself. I would also
contract with one of those individuals will be. In that situa-
ask that patient about his or her decision-making process
tion, you will not be dealing with a patient in the same state
to determine if the patient tends to make snap decisions.
as when you wrote the contract with him or her. We should
When treating somebody new, I try to be careful about
try to discuss the patient's state of mind with an infor-
understanding those issues and where they fit into the
mant-a spouse, close friend, or, in the case of a child or
patient's life and try to explore them in a nonjudgmental
adolescent, a parent. Certainly in the case of an adolescent,
if you are able to get information from a parent that the pa-
In some situations, even with patients I think I know
tient has been acting strangely, more hostile, or more
well, I will ask directly about impulsivity. Patients have
irritable since the medication was started, that would be
surprised me with their answers, especially those whom I
see as nonimpulsive but who see themselves as impulsive
Dr. Davidson: It is important to involve a significant
or report times in their life when they have been impulsive.
other to determine if there have been changes in behavior.
Disclosure of off-label usage: The chair has determined that, to the best
Table 6. Web Sites With Information Aboutthe
of his knowledge, bupropion, citalopram, escitalopram, mirtazapine,
U.S. Regulatory Actions onAntidepressants
nefazodone, paroxetine, sertraline, venlafaxine, and fluvoxamine are not
Antidepressant use in children, adlescents, and adults:
approved by the U.S. Food and Drug Administration for the treatment of
http://www.fda.gov/cder/drug/antidepressants/default.htm
pediatric depression. If you have questions, contact the medical affairs department of the manufacturer for the most recent prescribing
FDA statement regarding the antidepressant Paxil for the
http://www.fda.gov/bbs/topics/ANSWERS/2003/ANS01230.html
From the Department of Family Medicine, Boston Medical Center,
Antidepressant medications for children; information for parents
Boston, Mass. (Dr. Culpepper); the Department of Psychiatry and
Behavioral Sciences, Duke University Medical Center, Durham, N.C. (Dr. Davidson); the Department of Community and Family Medicine,
http://www.nimh.nih.gov/press/StmntAntidepmeds.cfm
Dartmouth Medical School, Hanover, N.H. (Dr. Dietrich); the Depart-
ment of Medicine, Regenstrief Institute, Inc., and Indiana University,
Indianapolis (Dr. Kroenke); the Department of Psychiatry, University of Florida, Gainesville (Dr. Goodman); and the Department of Family Medicine, University of Michigan Medical Center, Ann Arbor (Dr. Schwenk).
Dr. Culpepper: Is impulsivity a steady state or is it
In the spirit of full disclosure and in compliance with all ACCME
Dr. Davidson: It can change and, in my experience,
Essential Areas and Policies, the faculty for this CME activity was
SSRIs do alter impulsivity. They tend to control it rather
asked to complete a full disclosure statement. The information received is as follows: Dr. Culpepper is a consultant for Cephalon, Forest, Eli
than loosen it. However, we need to ask patients not only
Lilly, Pfizer, Somerset, and Wyeth. Dr. Davidson has received speaker
about suicidal impulses but aggressive impulses in gen-
fees from Solvay, Pfizer, GlaxoSmithKline, Wyeth, American Psychiatric Association, Forest, and Eli Lilly; is a scientific advisor for
eral, and we need to monitor patients closely to determine
Solvay, Pfizer, GlaxoSmithKline, Forest, Eli Lilly, Ancile, Roche,
how antidepressant treatment changes impulsivity in each
Novartis, Organon, Boehringer Ingelheim, UCB Pharma, Pharmacia,
Johnson & Johnson, Boots, Bristol-Myers Squibb, Cephalon, Nutrition 21, and Sanofi-Synthelabo; has received research support from Pfizer,
Dr. Culpepper: We as physicians must of course avoid
Solvay, Eli Lilly, GlaxoSmithKline, Wyeth, Organon, Forest, Pure
doing harm to our patients with the treatments we pre-
World, Allergan, Nutrition 21, Bristol-Myers Squibb, UCB Pharma, and
scribe. However, we must balance that with the possibility
Cephalon; has had drug supplied for NIH and other studies by Eli Lilly, Schwabe Pharmaceutical, Pure World, and Pfizer; and has received
of inflicting harm by withholding possibly beneficial or
royalties from MultiHealth Systems, Guilford Publications, American
lifesaving medications. The points we have emphasized
Psychiatric Association, and Penguin Putnam. Dr. Dietrich is on the speakers/advisory boards for Forest, Pifzer, and Wyeth. Dr. Goodman
here are neither new nor ominous, but reflect good clini-
is an employee of the University of Florida Department of Psychiatry,
cal practice: begin antidepressant treatment carefully,
has received grant/research support from Eli Lilly, Forest,
monitor patients closely, and watch for signs of untoward
GlaxoSmithKline, Pfizer, and Wyeth; and is a consultant/speaker for Bristol-Myers Squibb, Eli Lilly, Forest, Janssen, Pfizer, Roche, and
side effects, worsening symptoms, and increased
Solvay. Dr. Kroenke has received grant/ research support from Eli Lilly
suicidality. More information about the FDA advisory and
and Wyeth, has received honoraria from Pfizer, and is on the
regulatory action in the United States can be found at the
speakers/advisory board for Eli Lilly. Dr. Schwenk is a consultant for Eli Lilly.
Drug names: bupropion (Wellbutrin and others), citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac and others), mirtazapine (Remeron and others), nefazodone (Serzone and others), paroxetine (Paxil), sertraline (Zoloft), venlafaxine (Effexor).
For the CME Posttest for this article, see pages 885-8S7.
For more CME activities, visit---------------
----www.psychiatrist.com/cmehome
Psychological Problems Among Immigrants Sajjan Singh Bajwa, Ph.D. * * Formerly Professor, Khalsa College Amritsar and Asst. Professor, University of Southern California : 1461 W. Nancy Lane, Porterville. CA 93257. (USA) Thoughts give rise to desires, desires shape actions, actions become habits, and habits make character. All desires may or may not be fulfilled. The satisfied desires
28546A Iss 04-05 Lin Lot.ps - 5/4/2005 8:26 AMby mouth. If you get Lindane Lotion in your mouth or swallow LindaneLotion, call your area Poison Control Center right away and getemergency help. What is Lindane Lotion? Lindane Lotion is a medicine that is used to treat scabies. It kills scabiesand their eggs. Scabies are very small bugs that crawl under your skin, layeggs, and cause severe itch
 We are pleased to publish an offering from
our sister publication The Primary Care
Companion to The Journal of Clinical
Psychiatry about a topic of high importance to
all physicians. This special commentary is
Larry Culpepper. M.D.; Jonathan R. T. Davidson, M.D.;
the first independent project undertaken by
Allen J. Dietrich, M.D.; Wayne K. Goodman, M.D.; Kurt
Kroenke, M.D.; and Thomas L. Schwenk, M.D.
interests between psychiatry and primary
uicide is a tragic but not uncommon outcome to psychiatric illness.
The risk and rate of suicide among those who are mentally ill are
published in Prim Care Companion J Clin
higher than among the general population, and much effort has been
made by researches and clinicians in both psychiatry and primary care to
find ways to prevent suicide in these patients. However, reports that anti-depressant use can be associated with an increase in suicidal thoughts and behavior are cause for concern and have resulted in the public health
advisory issued by the U.S. Food and Drug Administration (FDA) in
March 2004. This advisory contained warnings relevant to 10 popular
antidepressant agents (Table 1): for a summary of the warning information
Issues Involved in the FDA's Assessment of
We are pleased to publish an offering from
our sister publication The Primary Care
Companion to The Journal of Clinical
Psychiatry about a topic of high importance to
all physicians. This special commentary is
Larry Culpepper. M.D.; Jonathan R. T. Davidson, M.D.;
the first independent project undertaken by
Allen J. Dietrich, M.D.; Wayne K. Goodman, M.D.; Kurt
Kroenke, M.D.; and Thomas L. Schwenk, M.D.
interests between psychiatry and primary
uicide is a tragic but not uncommon outcome to psychiatric illness.
The risk and rate of suicide among those who are mentally ill are
published in Prim Care Companion J Clin
higher than among the general population, and much effort has been
made by researches and clinicians in both psychiatry and primary care to
find ways to prevent suicide in these patients. However, reports that anti-depressant use can be associated with an increase in suicidal thoughts and behavior are cause for concern and have resulted in the public health
advisory issued by the U.S. Food and Drug Administration (FDA) in
March 2004. This advisory contained warnings relevant to 10 popular
antidepressant agents (Table 1): for a summary of the warning information
Issues Involved in the FDA's Assessment of 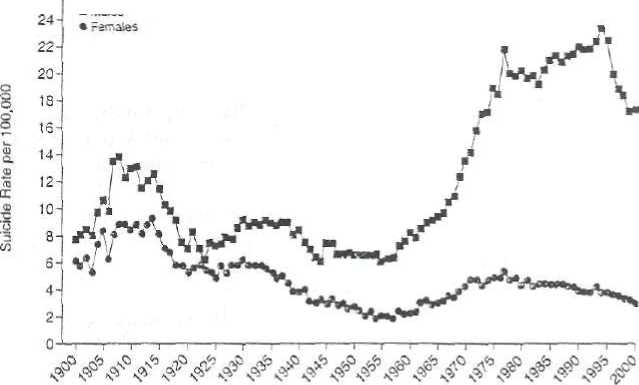 Figure I. Changes in Youth (aged 15-24 years) Suicide Rates in the United States During the 20th Century"
"Modified from David Shaffer's slide presentation "Suicide and "Related Problems in. Adolescents," given at the Feb. 2.
2004, meeting of the Psychopharmacologic Advisory Committee and the Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee of the U.S. Food and Drug Administration [FDA]. Available on the FDA Web site at: http://www.fda.gov/ohrms/dockets/ac/04/slides/4006S l-03-Shaffer.htm.
Dr. Kroenke: I would have a conversation with the pa-
Figure I. Changes in Youth (aged 15-24 years) Suicide Rates in the United States During the 20th Century"
"Modified from David Shaffer's slide presentation "Suicide and "Related Problems in. Adolescents," given at the Feb. 2.
2004, meeting of the Psychopharmacologic Advisory Committee and the Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee of the U.S. Food and Drug Administration [FDA]. Available on the FDA Web site at: http://www.fda.gov/ohrms/dockets/ac/04/slides/4006S l-03-Shaffer.htm.
Dr. Kroenke: I would have a conversation with the pa-