L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Untitled
European Journal of Cardio-Thoracic Surgery Advance Access published December 31, 2012
European Journal of Cardio-Thoracic Surgery 0 (2012) 1-6
Measurement of extravascular lung water following human brain
death; implications for lung donor assessment and transplantation
Rajamiyer V. Venkateswarana,*, Vamsidhar Dronavallia, Val Patchellb, Ian Wilsona, Jorge Mascaroa,
a Department of Heart and Lung Transplantation, University Hospital Birmingham NHS Foundation Trust, Birmingham, UKb Department of Physiology, Division of Medical Sciences, University of Birmingham, Birmingham, UK
* Corresponding author. Department of Cardiothoracic Surgery and Transplantation, University Hospital South Manchester NHS Foundation Trust,
Wythenshawe Hospital, Southmoor Road, Manchester M23 9LT, UK. Tel: +0161-291-2509; fax: +0161-291-2092; e-mail: rajamiyer.venkateswaran@uhsm.nhs.uk(R.V. Venkateswaran).
Received 5 March 2012; received in revised form 15 August 2012; accepted 7 September 2012
OBJECTIVES: The measurement of extravascular lung water could aid the assessment and guide the management of potential lungdonors following brain death. We therefore sought to validate a single indicator thermodilution extravascular lung water index (EVLWI-T) measurement using gravimetry and to assess the impact and clinical correlates of elevated EVLWI-T in potential lung donors andtransplant recipients.
METHODS: In a prospective study, we measured serial EVLWI-T and haemodynamic and oxygenation data in 60 potential lung donors. To validate the EVLWI-T measurement, we measured in vivo thermodilution EVLWI (EVLWI-T) and gravimetric ex vivo EVLWI (EVLWI-G)in donor lungs rejected for transplant using the Holcroft and Trunkey modification of Pearce's method. We assessed the clinical corre-lates of elevated lung water and measured interleukin-8 and hepatocyte growth factor in bronchoalveolar lavage (BAL) fluid.
RESULTS: The mean EVLWI-T (n = 60) was 9.7 (4.5) ml kg−1, being >7-10 ml kg−1 in 23/60 and >10 ml kg−1 in 16/60 potential donors. Donor lungs with EVLWI >10 ml kg−1 were more likely to be receiving norepinephrine (P = 0.04), have higher pulmonary capillarywedge pressures (P = 0.008), be unsuitable for transplantation (P = 0.007) and, if transplanted, have worse survival (P = 0.04). Lungs submitted to gravimetric analysis [n = 20 in 11 donors (9 double and 2 single)] had EVWLI-T of 10.8 (2.7) and EVLWI-G was 10.1(2.5). There was a strong correlation between EVLW-T and EVLW-G (r = 0.7; P = 0.014), but EVLWI-T over-predicted the EVLWI-G by
1 ml kg−1 (EVLW-T = 1.05 × EVLW-G). Cytokine levels in BAL fluid were elevated.
CONCLUSIONS: Elevated lung water is found in >50% of potential lung donors, predicts lung suitability for transplant and may adverse-ly affect recipient outcome. Although EVLWI-T intrinsically overestimates gravimetric lung water, its measurement may aid the assess-ment of organ suitability. Lung water accumulation and the proinflammatory response may both be targets for modifying therapy.
Keywords: Lung water • Extravascular lung water • Gravimetric lung water • Lung transplantation • Donor management
very significant increases in lung water observed immediately aftertransplantation []. The measurement of EVLW could thus be an
In the circumstances of brain death, extravascular lung water
additional facile and real-time method of assessment of potential
(EVLW) could increase due to direct lung injury associated with
the cardiovascular events of coning [and secondary effects
EVLW can be measured in different ways including a single
related to proinflammatory response or cardiac dysfunction ].
indicator trans-pulmonary thermodilution technique based on
Each of these could be exacerbated by over-zealous fluid re-
the Stewart-Hamilton principle [, ]. Using this thermodilution
placement. Current, in vivo assessment of donor lungs is inexact
technique, the EVLW, indexed to predicted body weight (PBW;
and reliant on donor history, chest-X-ray evaluation, arterial and
extravascular lung water index (EVLWI-T)), has a normal range of
pulmonary venous blood gas measurement, bronchoscopy and
3-7 ml kg−1 and values >10 ml kg−1 are believed to indicate
direct inspection [, ]. As in other clinical scenarios, significant
significant lung water excess [and predict adverse outcome
lung water increases might precede clinical, radiological and oxy-
genation manifestations of lung oedema and could potentiate the
Early EVLW studies, using a thermal dye double indicator
dilution technique suggested potential clinical utility in brain
Prof. Robert Bonser has unfortunately passed away after this paper was
-lung donors [], but the single indicator
technique has not been investigated or validated in this setting.
The Author 2013. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
In a previous report, we found that potential donor lungs
identified during assessment at direct inspection. Interleukin-8
deemed unsuitable for transplantation had higher EVLWI-T. The
(IL-8) and hepatocyte growth factor (HGF) as possible markers of
aims of the current study were therefore to validate the single
lung injury were measured in a single thaw cycle of the BAL
indicator thermodilution measurement against gravimetric meth-
supernatant sample using commercially available ELISA kits
odology in patients following brain death, and to assess the clin-
(Quantikine® by R&D Systems, Inc., MN, USA). As the kits were
ical and haemodynamic correlates of EVLWI-T measurements
not previously validated for use on BAL samples, for each of the
markers, spike/ recovery and linearity experiments were per-formed based on the manufacturer's protocol (R&D Systems,Inc.), ensuring measurement accuracy up to maximal alloweddilution.
Donor lungs for transplantation were flush perfused with a
single pulmonary artery flush of blood-based pneumoplegia
This prospective observational study was approved by a multi-
(Ringer's lactate 700 ml, human albumin solution (20%) 200 ml,
centre research ethics committee, and informed consent was
mannitol solution (20%) 100 ml, sodium heparin 10 000 units,
obtained from the next of kin of all participating donors. We
venesected donor blood 300 ml, citrate/phosphate/dextrose
performed EVLWI-T measurements using a single thermal indi-
buffer 56 ml and a single dose of epoprostenol infusion (0.5 mg
cator technique in brainstem dead potential lung donors
in 20 ml (Flolan; GlaxoSmithKline UK, Ltd)) and retrieved as a
defined as a donor with a PaO2/fractional inspired oxygen (FiO2)
whole block after explanting the donor heart. The trachea was
ratio at initial assessment of ≥200 mmHg, provided available
stapled after expansion of both lungs, and the block or individual
chest radiographs did not demonstrate gross parenchymal
lung transported in 4°C Ringer's lactate solution to the transplant
change. Demographic and clinical data, including time of coning
(detection of fixed dilated pupils and arterial blood pressuresurge) were recorded and arterial blood samples drawn for (i)blood gas measurements at fractional inspired oxygen (FiO2) 1.0
and 5 cmH2O positive end-expiratory pressure and (ii) for bio-marker analysis. A femoral arterial thermodilution catheter
Specific, additional next-of-kin consent was requested to retain
(PiCCO, Pulsion Medical UK, Ltd) was then inserted for the
lungs not accepted for transplantation for gravimetric lung water
measurement of EVLW and pulmonary vascular permeability
assessment. Gravimetric measurement of EVLW was determined
(PVP) both indexed (I) to PBW according to the formulae:
using the Holcroft and Trunkey modification of the Pearcemethod []. Peripheral venous (5 ml) and pulmonary venous ef-
Females : 45:5 þ 0:91½heightðcmÞ À 152:4
fluent blood (10 ml) were collected prior to retrieval of lungs forhaemoglobin estimation. Lungs were then retrieved in a standard
Males : 50:0 þ 0:91½heightðcmÞ À 152:4
manner, but without pneumoplegia or epoprostenol infusion
The underlying principles of this lung water assessment have
and transported, inflated at 4°C in Ringer's lactate solution.
been previously reported [The pulmonary vascular permeabil-
Within 8 h, lung blocks were separated, and non-parenchymal
ity index (PVPI) is the EVLW to pulmonary blood volume ratio
tissue excised and weighed. Large representative samples from
(normal range 1-3 kg−1). Elevated EVLW with a low PVPI implies
upper and lower lobes were weighed and then homogenized
a greater pulmonary blood volume and hydrostatic oedema,
with a known amount of distilled water and centrifuged at
whereas a high EVLW with a high PVPI implies permeability
12 000 rpm for 30 min at 4°C. The wet weights of supernatant,
oedema. A Swan-Ganz catheter was also inserted, allowing the
lung sediments and the pulmonary venous blood were obtained.
measurement of pulmonary capillary wedge pressure (PCWP)
Haemoglobin levels from the pulmonary venous effluent blood
and supernatant samples were measured. Supernatant, blood
A bronchoscopy was performed to assess anatomy, confirm
and the lung sediments were then freeze dried for 72 h and
endotracheal tube placement, aspirate secretions, and to obtain
weighed again to obtain their dry weight. EVLW was then calcu-
bronchoalveolar lavage (BAL) specimens. Blood and BAL speci-
lated, linearly extrapolated to the total lung weight and indexed
mens were kept on ice until return to the transplant centre
where they were immediately processed. Blood samples werecentrifuged and serum then frozen at −80°C for later analysis. One aliquot of BAL fluid was despatched for microbiological
culture and the centrifuged supernatant of a second specimenfrozen at −80°C for later cytokine analysis. ABG, EVLWI and PVPI
Data were analyzed using SPSS v15.0 (Chicago, IL, USA) and
measurements were obtained at baseline, repeated after bron-
STATA (Release 10; Stata Corp., College Station, TX). Continuous
choscopy, 1 h thereafter and immediately preretrieval.
data were assessed for normality and are presented as mean
After initial measurements and BAL, donors received either
(standard deviation) or median (25th, 75th quartiles). Normally
T3, methylprednisolone, both T3 and MP or placebo (dextrose
distributed variables were compared using the paired or inde-
5%) in a 1:1:1:1 randomization as previously described [
pendent t-test as appropriate. Skewed data were tested using
Details of blinding, randomization, donor management, a
non-parametric tests (Mann-Whitney and Kruskal-Wallis test).
CONSORT flow diagram and hormonal group allocation out-
Categorical data were analyzed using Chi-square and Fisher's
comes for this trial have been previously reported [Lung
suitability for transplantation was predefined as an arterial PaO2/
Comparison between gravimetry and thermodilution was per-
FiO2 ≥300 mmHg immediately prior to retrieval without lung
formed using Spearman's correlation and Bland-Altman analysis.
trauma, aspiration, infection or non-recruitable atelectasis being
We analysed donor EVLWI-T and corresponding lung EVLWI-G
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
(averaged if both lungs were available for gravimetric analysis).
Clinical and laboratory data according to EVLWI-T dichotomized
The receiver operating curve characteristic for the ability of
as ≤ or >10 ml kg−1 are shown in Table. High EVLW-T donors
EVLWI-T to predict lung suitability for transplantation at retrieval
had higher PVPI, higher PCWP and were more likely to be re-
assessment is reported as area under the curve (AUC; standard
ceiving a higher dose of norepinephrine and less likely to be
error). Statistical significance was assigned when P < 0.05, and all
suitable for transplantation at end inspection. Positive BAL
culture rates were not different between lung water groups.
Additionally, BAL levels of IL-8 [1472 (223, >2000) vs 2000 (663,
>2000) pg ml−1] and HGF [325 (125, 1160) vs 402 (222-1707) pg
ml−1; P = 0.47] were observed for the ≤10 and >10 ml kg−1
groups, respectively. IL-8 levels were highly elevated and were
Sixty donors, median age 47 (36, 56) years, underwent the in
beyond the measurable range despite maximal allowed dilution
vivo studies (Table ). The mean initial PaO2/FiO2 ratio was 396
(79) mmHg. Donors commenced investigations 2 (0.5, 3.5) h
Overall, both EVLWI-T and PVPI increased significantly
after consent, within 12.5 (8.1) h of coning. During a manage-
between initial and preretrieval measurements from 9.7 (4.5) to
ment period of 6.9 (1.2) h, donors received limited amounts of
10.8 (5.2); P = 0.009 and 2.4 (0.9) to 2.7 (1.2); P = 0.025, respect-
fluid [376 (353) ml of colloid and 27 (94) ml of crystalloid].
ively, while the PaO2/FiO2 ratio fell [397 (78) to 359 (126);
P = 0.028] and PCWP increased [8.4 (4.9) to 11.1 (4.2); P < 0.001]. On receiver operating characteristic curve analysis, initial EVLWI
EVLWI-T and gravimetric lung water validation
[AUC = 0.67 (0.07); 95% CI 0.53, 0.81; P = 0.025] (Fig. was pre-dictive of suitability at final inspection with a positive and nega-
Consent was obtained in 11 donors (20 lungs; 9 lung pairs and 2
tive predictive value of 72 and 63%, respectively.
single lungs) for gravimetric analysis. When comparing techni-
A total of 27 lung transplants were performed from the study
cohort; 30-day survival (60%) was lower in recipients of lungs
before lung explantation were considered. The gravimetric lung
with EVLWI-T >10 ml kg−1 (n = 5); P = 0.03 vs those with lower
study donors had a similar EVLWI-T [10.8 (2.7)] when compared
with others [10.6 (5.4) ml kg−1], but as expected, a lower PaO2/FiO2 ratio (265 (135) vs 373 (111) mmHg) than non-gravimetrically studied lungs. There was strong, direct correlation
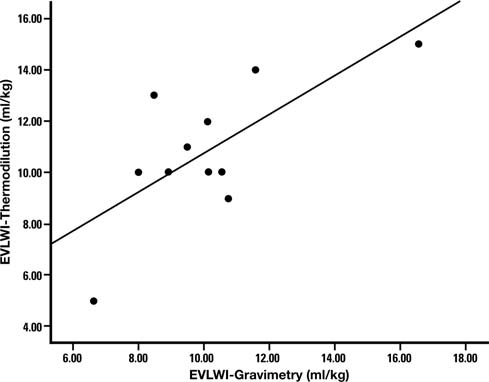
between EVLWI-T and EVLWI-G (Fig. ; r = 0.7; Spearman's cor-relation P = 0.014; regression analysis EVLW-T = 1.05 × EVLW-G)
Following transplantation, there is a disturbing incidence (15-
with modest over-prediction [Bland-Altmann analysis of 0.5
35%) of post-transplantation lung injury with impaired gas ex-
(2.1) ml kg−1] and increased positive bias with higher EVLWI
change and pulmonary infiltrates and worse outcome
measurements (Fig. The upper and lower limits of agreement
Increased lung water occurs uniformly [Our study suggests
(±2 standard deviations) were 4.6 and −3.7 ml kg−1, respectively.
that the process of oedema generation begins in the donor. Wehave demonstrated that EVLWI-T is elevated (>7 ml kg−1) in themajority of potential lung donors following brain death and is
6 h prior to final inspection, predicts the ultimate suit-
ability of lungs for transplantation and recipient outcome.
The initial EVLWI-T was 9.7 (4.5) ml kg−1; 85% (51/60) donors
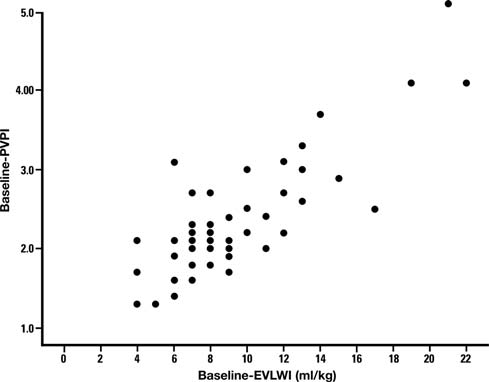
had EVLWI-T >7 ml kg−1, with 27% (16/60) having values >10 ml
methods (EVLWI-T) have been shown to correlate well with lung
kg−1. PVPI values rose in parallel with increasing EVLWI-T (Fig.
Characteristics of 60 potential lung donors
Data are presented in mean (standard deviation), median (25th, 75thpercentiles) or number/denominator (%). CNS: central nervous system.
Figure 1: Correlation between EVLWI measurement by thermodilution andgravimetry (r = 0.7; Spearman's correlation P = 0.002).
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Figure 2: Bland-Altman plot demonstrating limits of agreement between EVLWI measurement by thermodilution and gravimetry. EVLWI-T over-predicted theEVLWI-G and there was a positive bias which increased with higher EVLWI-T. However the limits of agreement values lie between the two standard deviation.
although the validity of PVPI as an index of permeabilityoedema has not been validated. All the mechanisms describedcould lead to pulmonary oedema and worsening lung function,and our data are consistent with findings in lungs rejected fortransplantation [The higher PCWP in the >10 ml kg−1 groupis consistent with greater overall fluid overload or associated leftventricular dysfunction.
The huge circulating levels of catecholamines during the
'storm' of brainstem death may provoke pulmonary endothelialinjury and combined hydrostatic and permeability oedema. Thereafter, vasoparetic hypotension is commonly treated by NEinfusion, a potent but cardiotoxic α-adrenergic agonist. Donorpressor support with NE has been associated with a worse prog-nosis in heart and lung transplantation and inferior post-transplant gas exchange. In our study, more donors in theEVLWI-T >10 ml kg−1 group were receiving NE at higher dosage. Higher NE exposure could certainly influence lung water viahydrostatic mechanisms that increase fluid filtration, includingpost-capillary vasconstriction and cardiac dysfunction with
Figure 3: Scatter plot of EVLWI-T and PVPI.
The epithelial Na+/K+ channels in alveolar epithelium have an
water measured by gravimetry (EVLW-G) , , ]. A number of
important role in the clearance of excessive fluid from the alveo-
experimental studies have allowed validation of the single indica-
lar space. Alveolar fluid clearance (AFC) mechanisms are known
tor thermodilution method used in this study vs gravimetric
to be maintained following brainstem death and retrieval and
measurement , In each study, EVLWI-T has been
may respond to pharmacological manipulation. Both thyroid
shown to over-predict EVLWI-G by 2-5 ml kg−1. In our study, the
hormone and steroids may up-regulate AFC and could be of
first to attempt to validate the measurement in potential donor
benefit in this clinical scenario [, ]. However, we previously
lungs, we noted a similar over-prediction of gravimetric values, a
reported that in this cohort, T3 had no effect on EVLWI-T while
positive bias that increases with higher EVLWI values, but which
MP attenuated the increased Δ-EVLWI-T observed in non-
may not limit the clinical value of this measurement.
treated donors. Early steroid administration is reported to
Lung water may increase in donor lungs by various mechan-
improve oxygenation and yield and, in this regard, augmentation
isms of injury such as trauma, aspiration, infection, fluid overload
of AFC rather than an anti-inflammatory effect may be the dom-
and ventilatory barotrauma. These may occur before or after
brain death, and donor smoking may be an additional risk
Importantly, our finding of elevated EVLWI-T in >50% donors
factor. Also, during the circulatory changes associated with brain
provides an opportunity for modulation using diuretics to coun-
death, haemodynamic shear forces and pro-oedematous hydro-
teract fluid overload and nebulized β-adrenergic agonists to
static pressures may cause direct injury. Each of these modes of
augment AFC. As post-transplantation increases in EVLWI occur
injury may be further exacerbated by a proinflammatory
uniformly following transplantation commencement of AFC
post-BSD environment, and our finding of elevated PVPI in
augmentation in the donor holds promise as a protective strat-
higher lung water donors suggests that this may be occurring
egy [Post-transplantation AFC manipulation has been shown
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Characteristics of donors and transplant outcome according to initially measured lung water content
The assessment time represents the period between initial and final measurements. The prefix Δ indicates the change in measurement between final andinitial sampling. Lungs matching suitability indicates those attaining the predefined transplant suitability criteria (see text). PVPI: pulmonary vascular permeability index: PCWP: initial pulmonary capillary wedge pressure.
to be associated with rapid resolution of hypoxia and improve-ment in radiological changes ].
Our study suggests that the measurement of EVLWI-T may be
a facile tool that may improve donor care. It may guide donorfluid management and prompt measures to improve AFC. Thestudy was performed prior to the widespread introduction of ex
vivo lung resuscitation ], but we speculate that the identifica-tion of adverse lung water measurements, rather than being aprompt for lung rejection, may allow direct transfer to lungreconditioning.
Our study has a number of limitations. Although our sample sizeis larger than many laboratory experimental studies, the hetero-geneity of the population may have affected our findings. Gravimetric validation was performed on lungs rejected fortransplantation that had worse gas exchange than those trans-planted. Caution must therefore be advised when extrapolatingthese data clinically. As patients were transplanted in a numberof centres, we used recipient survival as a surrogate measure of
Figure 4: Receiver operating curve characteristic assessing lung suitability and
graft function and cannot report whether differences in outcome
extravascular lung water index. The area under the curve is 0.67 (standard
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
In conclusion, we have validated the simple measurement of
[11] Mihm F, Feeley T, Rosenthal M, Lewis F. Measurement of extravascular
EVLWI by a single indicator thermodilution technique in post-
lung water in dogs using the thermal-green dye indicator dilutionmethod. Anesthesiology 1982;57:116-22.
brainstem death potential lung donors. Measurement many
[12] Venkateswaran RV, Patchell VB, Wilson IC, Mascaro JG, Thompson RD,
hours prior to retrieval may aid the prediction of organ suitabil-
Quinn DW et al. Early donor management increases the retrieval rate of
ity and recipient outcome. Elevated EVLWI-T represents a thera-
lungs for transplantation. Ann Thorac Surg 2008;85:278-86.
peutic target for modifying therapy during optimization.
[13] Holcroft JW, Trunkey DD. Extravascular lung water following hemor-
rhagic shock in the baboon: comparison between resuscitation withRinger's lactate and Plasmanate. Ann Surg 1974;180:408-17.
Conflict of interest: none declared.
[14] Ware LB, Golden JA, Finkbeiner WE, Matthay MA. Alveolar epithelial
fluid transport capacity in reperfusion lung injury after lung transplant-ation. Am J Respir Crit Care Med 1999;159:980-8.
[15] Lee JC, Christie JD. Primary graft dysfunction. Proc Am Thorac Soc 2009;
[16] Michard F. Bedside assessment of extravascular lung water by dilution
[1] Mutoh T, Kazumata K, Ajiki M, Ushikoshi S, Terasaka S. Goal-directed
methods: temptations and pitfalls. Crit Care Med 2007;35:1186-92.
fluid management by bedside transpulmonary hemodynamic monitor-
[17] Sturm J. Development and significance of lung water measurement in
ing after subarachnoid hemorrhage. Stroke 2007;38:3218-44.
clinical and experimental practice. In: Lewis FR, Pfeiffer UJ (eds). Practical
[2] Avlonitis VS, Wigfield CH, Golledge H, Kirby JA, Dark JH. Early hemo-
Applications of Fiberoptics in Critical Care Monitoring. Berlin: Springer,
dynamic injury during donor brain death determines the severity of
primary graft dysfunction after lung transplantation. Am J Transpl 2007;7:
[18] Katzenelson R, Perel A, Berkenstadt H, Preisman S, Kogan S, Sternik L
et al. Accuracy of transpulmonary thermodilution versus gravimetric
[3] Fisher AJ, Donnelly SC, Pritchard G, Dark JH, Corris PA. Objective assess-
measurement of extravascular lung water. Crit Care Med 2004;32:
ment of criteria for selection of donor lungs suitable for transplantation.
[19] Kirov MY, Kuzkov VV, Kuklin VN, Waerhaug K, Bjertnaes LJ. Extravascular
[4] Ware LB, Neyrinck A, O'Neal HR, Lee JW, Landeck M, Johnson E et al.;
lung water assessed by transpulmonary single thermodilution and post-
CTD Network. Comparison of chest radiograph scoring to lung weight as
mortem gravimetry in sheep. Crit Care Med 2004;8:R451-8.
a quantitative index of pulmonary edema in organ donors. Clin
[20] Ware LB, Wang Y, Fang X, Warnock M, Sakuma T, Hall TS et al.
Assessment of lungs rejected for transplantation and implications for
[5] Perrin G, Roch A, Michelet P, Reynaud-Gaubert M, Thomas P, Doddoli C
donor selection. Lancet 2002;360:619-20.
et al. Inhaled nitric oxide does not prevent pulmonary edema after lung
[21] Minnear FL, Barrie PS, Malik AB. Effects of epinephrine and norepineph-
transplantation measured by lung water content. Chest 2006;129:1024-30.
rine infusion on lung fluid balance in sheep. J Appl Physiol 1981;50:
[6] Brown LM, Liu KD, Matthay MA. Measurement of extravascular lung
water using the single indicator method in patients: research and poten-
[22] Noda M, Suzuki S, Tsubochi H, Sugita M, Maeda S, Kobayashi S et al.
tial clinical value. Am J Physiol Lung Cell Mol Physiol 2009;297:L547-58.
Single dexamethasone injection increases alveolar fluid clearance in
[7] Sakka SG, Rühl CC, Pfeiffer UJ, Beale R, McLuckie A, Reinhart K et al.
adult rats. Crit Care Med 2003;31:1183-9.
Assessment of cardiac preload and extravascular lung water by single
[23] Folkesson HG, Norlin A, Wang Y, Abedinpour P, Matthay MA.
transpulmonary thermodilution. Intensive Care Med 2000;26:180-7.
Dexamethasone and thyroid hormone pretreatment upregulate alveolar
[8] Sakka SG, Klein M, Reinhart K, Meier-Hellmann A. Prognostic value of
epithelial fluid clearance in adult rats. J Appl Physiol 2000;88:416-24.
extravascular lung water in critically Ill patients. Chest 2002;122:2080-6.
[24] Ware LB, Landeck M, Koyama T, Johnson E, Bernard GR, Lee JW et al. A
[9] Martin G, Eaton S, Mealer M, Moss M. Extravascular lung water in
randomized trial of nebulized albuterol to enhance resolution of pul-
patients with severe sepsis: a prospective cohort study. Crit Care 2005;9:
monary edema in 506 brain dead organ donors. J Heart Lung Transpl
[10] Berkowitz DM, Danai PA, Eaton S, Moss M, Martin GS. Accurate charac-
[25] Cypel M, Yeung JC, Liu M, Anraku M, Chen F, Karolak W et al.
terization of extravascular lung water in acute respiratory distress syn-
Normothermic ex vivo lung perfusion in clinical lung transplantation.
drome. Crit Care Med 2008;36:1803-9.
Hormones and Behavior 31, 145 – 158 (1997) Article No. HB971376 Hormonal and Experiential Correlates of Maternal Responsiveness during Pregnancy and the Puerperium in Human Mothers Alison S. Fleming Department of Psychology, University of Toronto, Erindale Campus,Mississauga, Ontario L5L 1C6, Canada Diane Ruble Department of Psychology, New York University, New York, New York 10012 H
This page to be retained by client Elderly Vaccination Subsidy Scheme (EVSS) 2011/12 Information about Seasonal Influenza Vaccination and Pneumococcal Vaccination Benefits of Getting Seasonal Influenza Vaccination and Pneumococcal Vaccination Infection of the airway such as those caused by seasonal influenza virus and pneumococcus is common. Once elders are infected, they are
 R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
(averaged if both lungs were available for gravimetric analysis).
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
(averaged if both lungs were available for gravimetric analysis).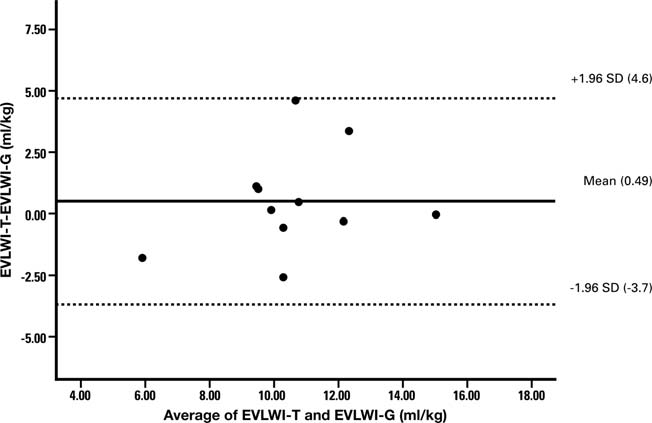
 R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Figure 2: Bland-Altman plot demonstrating limits of agreement between EVLWI measurement by thermodilution and gravimetry. EVLWI-T over-predicted theEVLWI-G and there was a positive bias which increased with higher EVLWI-T. However the limits of agreement values lie between the two standard deviation.
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Figure 2: Bland-Altman plot demonstrating limits of agreement between EVLWI measurement by thermodilution and gravimetry. EVLWI-T over-predicted theEVLWI-G and there was a positive bias which increased with higher EVLWI-T. However the limits of agreement values lie between the two standard deviation.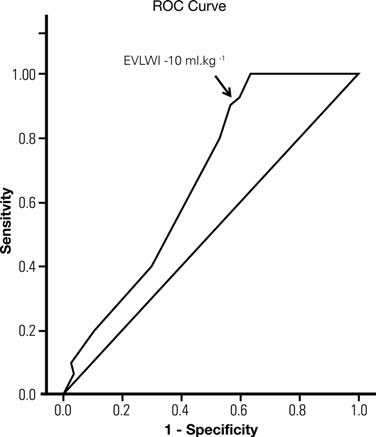 R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Characteristics of donors and transplant outcome according to initially measured lung water content
The assessment time represents the period between initial and final measurements. The prefix Δ indicates the change in measurement between final andinitial sampling. Lungs matching suitability indicates those attaining the predefined transplant suitability criteria (see text).
R.V. Venkateswaran et al. / European Journal of Cardio-Thoracic Surgery
Characteristics of donors and transplant outcome according to initially measured lung water content
The assessment time represents the period between initial and final measurements. The prefix Δ indicates the change in measurement between final andinitial sampling. Lungs matching suitability indicates those attaining the predefined transplant suitability criteria (see text).