L’ivermectine (Stromectol) est un antiparasitaire dont l’action repose sur la liaison sélective aux canaux chlore activés par le glutamate présents dans les cellules nerveuses et musculaires des parasites. Cette fixation entraîne une augmentation du flux de chlore, provoquant une hyperpolarisation et une paralysie irréversible. L’ivermectine est active contre la gale, l’onchocercose et certaines strongyloïdoses. Sa biodisponibilité orale est variable, augmentée par la prise alimentaire, et son élimination est principalement fécale via un métabolisme hépatique. Elle ne traverse pas la barrière hémato-encéphalique, ce qui limite les effets neurologiques chez l’homme. Les précautions concernent l’interaction avec les inhibiteurs du CYP3A4, ainsi que les réactions inflammatoires dues à la destruction massive des parasites. Dans les documents de référence, stromectol prix est associé à des protocoles précis adaptés aux différentes infestations, avec une attention particulière sur la sécurité d’emploi en cas d’immunodépression.
Bart d - lap nissen op script
Laparoscopic Anti Reflux Surgery Patient Information
1. What is Gastro-Oesophageal Reflux Disease?
Reflux disease (Gastro-oesophageal reflux disorder also known as
GORD) is a condition that results from the acid in the stomach going up
in to the Oesophagus (gullet) causing inflammation of the lower part of
Normally, this acid reflux is prevented by the sphincter in the lower
part of the oesophagus. In patients with reflux disease, this sphincter
which acts as valve does not function normally.
a) Heart Burn: A burning feeling in the upper abdomen. It can
travel through the chest and into the throat and neck.
b) Regurgitation: A warm salty, bitter taste in the mouth. It
occurs when stomach contents flow back into the mouth,
Dysphagia: Food is sometimes stuck in the oesophagus and
may be painful in swallowing. Always need to be investigated
a) Chest pain: Pain in the chest reflecting spasm in the
oesophagus and can mimic a heart attack.
b) Hoarseness: This can develop if the acid and or stomach
contents reach the mouth and throat.
Choking/ Wheezing: It may occur at night when stomach
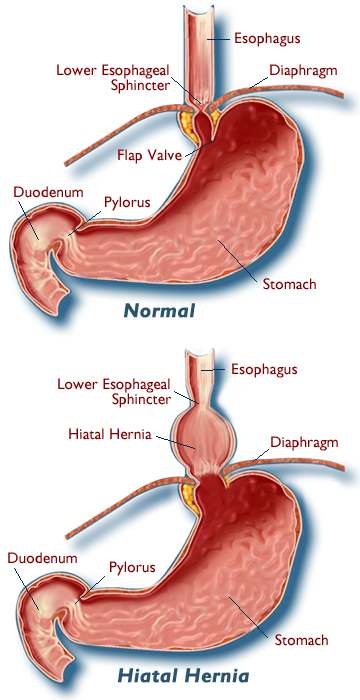
a) A weak lower oesophageal sphincter.
b) Hiatus Hernia: This occurs when part of the stomach bulges up
through the diaphragm and into the chest.
Hiatus hernia is common in the population but not everybody
with Hiatus hernia will suffer from GORD.
Other factors that may contribute to GORD are fatty foods,
smoking, chocolate, caffeine, alcohol, obesity and pregnancy.
The first step in treating GORD includes lifestyle and diet
modifications. These are usually very effective.
Try to limit or avoid foods that can exacerbate GORD (eg: alcohol).
Eat small Meals, avoid late evening meals, cut down or stop
smoking, lose weight, avoid tight fitting clothes.
Elevate the head of bed by placing blocks under the bedpost.
Antacids : Gaviscon is usually the first drug recommended to
relieve heartburn and other mild GORD symptoms. H2 blocker:
Cimetidine and Ranitidine, impede acid production.
Proton pump inhibitors or PPI: These drugs are extremely effective
at decreasing the 24-hour acid output by the stomach.
Omeprazole, Lansoprazole are commonly used PPI.
Anti-reflux procedures are used to treat GORD. They work by
strengthening the valve mechanism at the junction of the oesophagus
and stomach, thus preventing reflux of acid into the oesophagus.
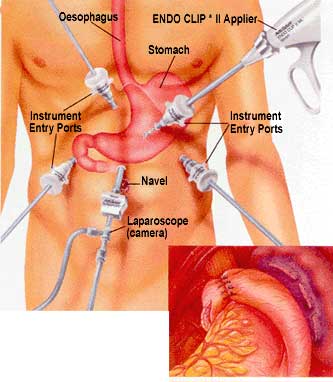
The procedure can be performed using keyhole (laparoscopic) or open
surgery. The advantage of keyhole surgery being quicker recovery time
and smaller scars. Indeed most operations are now performed as day
7. Patient selection for operation: Who needs this?
In majority of the cases this reflux disease can be successfully treated
with medication. Patients suitable for surgery are:
a) Poorly controlled symptoms despite medication. b) When medication fails to prevent potential complication of
Undesirable side effects from conventional medications and/
d) Young patients who do not wish to take medication for life. e) Patient with Barrett's oesophagus.
This operation requires general anaesthesia (patients are put to sleep).
All patients will be assessed in preoperative assessment clinic. Some
blood test, a chest x-ray and an ECG (heart trace) may be required
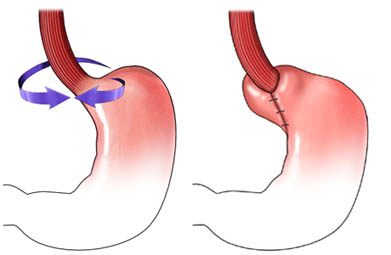
prior to surgery. The procedure most commonly performed is Laparoscopic Nissen
Fundoplication with repair of Hiatus Hernia. Usually it is completed
using keyhole surgery using 5 small incisions on the abdomen.
The Hiatus Hernia (defect in the diaphragm) is repaired with stitches.
Next the uppermost part of the stomach is wrapped loosely around the
lower part of the oesophagus and secured with stitches; this will
strengthen the valve at the bottom of the oesophagus and prevents
reflux of acid from the stomach into the oesophagus thereby
9.What Preparation do you need to take before operation?
A good shower the night before or morning of the operation is
recommended. Patients are advised not to eat or drink anything after
midnight the night before the operation. You can take some of your
medications with a sip of water in the morning of surgery. Medications
such as aspirin, warfarin, anti-inflammatory medications (such as
diclofenac) may need to be stopped temporarily prior to surgery. Do
not worry all preoperative medication issues will be discussed in the
10. The day of surgery and Hospital stay:
Patients are advised to arrive at the hospital the morning of the
operation. They will be reviewed by one of the team member and
Anaesthetists. The procedure is performed under general anaesthesia.
Most of the time the procedure will take ½ to 1 hr. You will be taken to
the recovery room until you are fully awake.
In the majority of cases patients are discharged home on the same day
(day-case surgery) or the following morning.
There are some risks and side effects associated with this operation
like any other surgical procedureComplications of anaesthesia are usually not common provided that
patients are fit otherwise. The Anaesthetist will discuss these prior to
Bleeding or bruising associated with the small skin incisions. Infections
in the operation site which is very rare. Deep vein thrombosis and
pulmonary embolism. This can occur after prolonged periods of
immobility. It is more common in patients that are overweight and/or
smoke. Early mobilisation, hydration and compression stockings lower
Complications specific to anti-reflux surgery:
Very rarely damage to the oesophagus, stomach or lung lining (Pleura)
Conversion to open surgery (Less than 1%).
Small risk of splenic injury and splenectomy (Less than 1%).
Very rarely severe complications may result in death. However, the risk
of serious complication is very small (about 1 in 1000, UK national
Difficulty swallowing: Most common, about 30% of patient experience
this after surgery, but usually temporarily for 4-6 weeks.
Abdominal bloating and flatulence: Very common. Caused by inability
to expel excess air in the stomach. This problem tends to get better
with time, but some degree of increased passage of wind often
remains. Indigestion - usually settles quickly.
Loss of Weight : Because of feeling full earlier some patients eat less
You will be allowed to begin to sip liquids a few hours after operation.
You should initially avoid all food with lumps, Very hot or very cold
food. Avoid breads, crackers, biscuits, pancakes and toast, carbonated
On day 2 - soft diet such as soup, yoghurt, custard etc is acceptable.
Try to eat slowly ideally over 1 hour period initially. You should take
plenty of drink to keep food moist. It is better to avoid tomato
products, peppermint, black pepper, caffeine, alcohol, onions, green
peppers, "gum chewing", fatty foods, beans, raw vegetables, fibre
supplements as these can be irritating.
Food may get stuck in the gullet. Take small sips of water and walk
round until the food moves down to stomach in this situation.
For first 2 weeks eat soft food (e.g steamed fish, mash potatoes) and
After 6 weeks you should be able to eat a regular diet. However,
people often find they are able to eat less than they used to.
14. When to seek medical attention following operation?
You will be reviewed in the outpatient clinic 6 weeks post operatively.
But one must seek urgent medical advice if there is (which is very rare)
1. High fever2. Bleeding3. Abdominal swelling that is increasing. 4. Pain that is not relieved by your medications5. Persistent nausea or vomiting6. Persistent cough or shortness of breath7. Purulent drainage (pus) from any of the wounds8. Redness surrounding any wound that is worsening or getting bigger9. Inability to swallow solids or drink liquids
Majority of the patients - almost 95%, remain symptom free and do not
require anymore anti acid medications after the procedure. Follow-up
indicates that 10 years after surgery, 80-85% of patients continue to
1. Wound Care: The five small wounds are closed with stitches that
dissolve and do not need to be removed. You can bath or shower
normally on next day after the operation.
2. Pain Control: Post-operative pain is generally mild and a simple
painkiller for 3-7 days usually helps.
3. Bowels and Bladder: You should not experience any difficulty in
opening your bowels or passing urine following your operation.
However, you may be prone to constipation when taking some
painkillers. Occasionally some patients suffer from diarrhoea after
their operation but this normally settles quickly.
You should expect to resume normal activities approximately 4 to 6
weeks following your surgery. Driving should be avoided until you can
perform an 'emergency stop' without hesitation. We suggest not driving
for at least 2 weeks (Please check with your insurance company). You
should avoid heavy lifting for 6 weeks as it increases the risk of
developing hernias through small wounds.
You will be given 2 weeks sick note for work if requested (which may
be extended by the GP if necessary). Any further queries please
contact Mr. Decadt's (Consultant Surgeon, Upper G.I) Secretary:
MEDLInC CLINICAL PATHWAYS: ABNORMAL LIVER FUNCTION TESTS What is normal varies by ethnic origin and age. The term "normal range" introduces further confusion, as the values reflect a statistical range and not a definition of what is not pathological. Results outside of these ranges, therefore, do not necessarily indicate disease. The first step is to evaluate the clinical context in
The work to be done in Haiti will be prioritized in cooperation with the Methodist Church of Haiti (EMH). In general, projects range from construction to medical missions, and can include community development and relationship-building activities (like Vacation Bible School, ESL Classes, Adult Education: Specific Skill training, Vocational Training). Additional projects are reviewed by an oversi
 9.What Preparation do you need to take before operation?
A good shower the night before or morning of the operation is
recommended. Patients are advised not to eat or drink anything after
midnight the night before the operation. You can take some of your
medications with a sip of water in the morning of surgery. Medications
such as aspirin, warfarin, anti-inflammatory medications (such as
diclofenac) may need to be stopped temporarily prior to surgery. Do
not worry all preoperative medication issues will be discussed in the
10. The day of surgery and Hospital stay:
Patients are advised to arrive at the hospital the morning of the
operation. They will be reviewed by one of the team member and
Anaesthetists. The procedure is performed under general anaesthesia.
Most of the time the procedure will take ½ to 1 hr. You will be taken to
the recovery room until you are fully awake.
9.What Preparation do you need to take before operation?
A good shower the night before or morning of the operation is
recommended. Patients are advised not to eat or drink anything after
midnight the night before the operation. You can take some of your
medications with a sip of water in the morning of surgery. Medications
such as aspirin, warfarin, anti-inflammatory medications (such as
diclofenac) may need to be stopped temporarily prior to surgery. Do
not worry all preoperative medication issues will be discussed in the
10. The day of surgery and Hospital stay:
Patients are advised to arrive at the hospital the morning of the
operation. They will be reviewed by one of the team member and
Anaesthetists. The procedure is performed under general anaesthesia.
Most of the time the procedure will take ½ to 1 hr. You will be taken to
the recovery room until you are fully awake.